Exhibit 99.1
![]()
MANAGEMENT’S DISCUSSION AND ANALYSIS OF THE FINANCIAL SITUATION AND OPERATING RESULTS – FOR THE THREE AND NINE-MONTH PERIODS ENDED DECEMBER 31, 2019 AND 2018
Introduction
This management’s discussion and analysis (“MD&A”) is presented in order to provide the reader with an overview of the financial results and changes to the financial position of Acasti Pharma Inc. and its wholly owned subsidiary Acasti Innovations AG, incorporated in December 2019 under the laws of Switzerland for the purpose of future development of the Corporation’s intellectual property (collectively referred to in this MD&A as “Acasti”, “the Corporation”, “we”, “us” and “our”) as at December 31, 2019 and for the three and nine-month periods then ended. This MD&A explains the material variations in the financial statements of operations, financial position and cash flows of Acasti for the three and nine-month periods ended December 31, 2019, and 2018.
Market data and certain industry data and forecasts included in this MD&A were obtained from internal corporation surveys, market research, and publicly available information, reports of governmental agencies and industry publications and surveys. We have relied upon industry publications as our primary sources for third-party industry data and forecasts. Industry surveys, publications and forecasts generally state that the information they contain has been obtained from sources believed to be reliable, but that the accuracy and completeness of that information is not guaranteed. We have not independently verified any of the data from third-party sources or the underlying economic assumptions they made. Similarly, internal surveys, industry forecasts and market research, which we believe to be reliable based upon our management’s knowledge of our industry, have not been independently verified. Our estimates involve risks and uncertainties, including assumptions that may prove not to be accurate, and these estimates and certain industry data are subject to change based on various factors, including those discussed under “Risk Factors” in this MD&A. While we believe our internal business research is reliable and the market definitions we use in this MD&A are appropriate, neither our business research nor the definitions we use have been verified by any independent source. This MD&A may only be used for the purpose for which it has been published.
In this MD&A, financial information is for the three and nine-month periods ended December 31, 2019 and 2018 and is based on the interim consolidated financial statements of the Corporation, which were prepared in accordance with International Accounting Standard (“IAS”) 34, Interim Financial Reporting, as issued by the International Accounting Standards Board (“IASB”). The Corporation applied the same accounting policies in the preparation of these condensed interim consolidated financial statements as those disclosed in note 3 of its most recent annual non-consolidated financial statements, except they include the new standards, and amendments to standards, which are effective for the period beginning on April 1, 2019 and have been adopted by the Corporation, and the application of IFRS 10 “Consolidation”. In accordance with its mandate, the Audit Committee of the Corporation’s Board of Directors reviews the contents of the MD&A and recommends its approval to the Board of Directors. The Board of Directors approved this MD&A on February 14, 2020. Disclosure contained in this document is current to that date, unless otherwise noted. Note that there have been no significant changes to the “Use of estimates and measurement uncertainty”, “Critical Accounting Policies”, and “Financial instruments” in comparison to those disclosed in the Corporation’s MD&A for the year ended March 31, 2019, filed with the securities regulatory authorities on June 26, 2019. Readers should carefully review and consider the risks and uncertainties described in the Corporation’s filings with securities regulators, as well as in its Annual Report on Form 20-F filed with securities regulatory authorities in the U.S. on June 26, 2019 and in Canada on July 4, 2019. The Corporation’s financial results are published in Canadian dollars. All amounts disclosed in this MD&A are in thousands of Canadian dollars, except share and per share amounts or unless otherwise indicated.
| 1 |
Additional information about the Corporation can be found on the SEDAR website at www.sedar.com or on EDGAR at www.sec.gov/edgar.shtml under Acasti Pharma Inc.
The Class A shares of the Corporation (“Common Shares”) are listed for trading on the TSX Venture Exchange and on the NASDAQ Capital Market exchange under the ticker symbol “ACST”.
We own or have rights to trademarks, service marks or trade names that we use in connection with the operation of our business. In addition, our name, logo and website names and addresses are our service marks or trademarks. CaPre® is our registered trademark. The other trademarks, trade names and service marks appearing in this MD&A are the property of their respective owners. Solely for convenience, the trademarks, service marks, tradenames and copyrights referred to in this MD&A are listed without the ©, ® and TM symbols, but we will assert, to the fullest extent under applicable law, our rights or the rights of the applicable licensors to these trademarks, service marks and tradenames.
FORWARD-LOOKING STATEMENTS
This MD&A contains information that may be forward-looking information within the meaning of Canadian securities laws and forward-looking statements within the meaning of U.S. federal securities laws, both of which we refer to in this MD&A as forward-looking information. Forward-looking information can be identified by the use of terms such as “may”, “will”, “should”, “expect”, “plan”, “anticipate”, “believe”, “intend”, “estimate”, “predict”, “potential”, “continue” or other similar expressions concerning matters that are not statements about the present or historical facts. Forward-looking information in this MD&A includes, among other things, information or statements about:
| · | our ability to conduct all required clinical and nonclinical trials for CaPre, including the timing and results of those trials; |
| · | the timing and outcome of our ongoing investigation regarding the unusually large placebo effect observed in the triglyceride topline results of our TRILOGY 1 Phase 3 clinical trial; |
| · | our ability to file a New Drug Application, or NDA, based on the results of our TRILOGY Phase 3 program; |
| · | whether the FDA may require additional clinical development work to support our NDA filing for CaPre; |
| · | our strategy, future operations, prospects and the plans of our management; |
| · | the regulatory plan, timeline, costs and results of our clinical and nonclinical trials for CaPre; |
| · | the timing and outcome of our meetings and discussions with the U.S. Food and Drug Administration, or FDA; |
| · | our planned regulatory filings for CaPre, and their timing; |
| · | our expectation that our Bridging Study results will support our plan to get authorization from the FDA to use the 505(b)(2) pathway with new chemical entity, or NCE, status towards an NDA approval in the United States; |
| · | the potential benefits and risks of CaPre as compared to other products in the pharmaceutical, medical food and natural health products markets; |
| · | our estimates of the size of the potential market for CaPre, unmet medical needs in that market, the potential for market expansion, and the rate and degree of market acceptance of CaPre if it reaches commercialization, and our ability to serve that market; |
| · | our anticipated marketing advantages and product differentiation of CaPre and its potential to become a best-in-class omega-3 (“OM3”) compound for the treatment of HTG; |
| · | the potential to expand CaPre’s indication for the treatment of high TGs (200-499 mg/dL); |
| · | the degree to which physicians would switch their patients to a product with CaPre’s target product profile; |
| · | our strategy and ability to develop, commercialize and distribute CaPre in the United States and elsewhere; |
| 2 |
| · | our ability to strengthen our patent portfolio and other means of protecting our intellectual property rights, including our ability to obtain additional patent protection for CaPre; |
| · | our expectation that following expiration of the license agreement with Neptune Wellness Solutions Inc. (formerly Neptune Technologies & Bioressources Inc.) (“Neptune”) we will not require any license from third parties to support the commercialization of CaPre; |
| · | the availability, consistency and sources of our raw materials, including krill oil; |
| · | our expectation to be able to rely on third parties to manufacture CaPre whose manufacturing processes and facilities are in compliance with current good manufacturing practices, or cGMP; |
| · | the potential for Omega-3 therapeutics, or OM3s in other cardiometabolic medicine indications; |
| · | our intention and ability to build a U.S. commercial organization and to successfully launch CaPre and compete in the U.S. market; |
| · | our intention and ability to complete development and/or distribution partnerships to support the commercialization of CaPre outside of the United States, and to pursue strategic opportunities to provide capital and market access; |
| · | our need for additional financing and our estimates regarding our future financing and capital requirements; |
| · | our expectation regarding our financial performance, including our revenues, profitability, research and development, costs and expenses, gross margins, liquidity, capital resources, and capital expenditures; and |
| · | our projected capital requirements to fund our anticipated expenses, including our research and development and general and administrative expenses, and capital expenditures. |
Although the forward-looking information in this MD&A is based upon what we believe are reasonable assumptions, you should not place undue reliance on that forward-looking information since actual results may vary materially from it. Important assumptions made by us when making forward-looking statements include, among other things, assumptions by us that:
| · | we are able to obtain the additional capital and financing we require; |
| · | we successfully and timely complete all required clinical and nonclinical trials necessary for regulatory approval of CaPre; |
| · | the timeline and costs for our clinical and nonclinical programs are not materially underestimated or affected by unforeseen circumstances; |
| · | CaPre is safe and effective; |
| · | we obtain and maintain regulatory approval for CaPre on a timely basis; |
| · | we are able to attract, hire and retain key management and skilled scientific and commercial personnel; |
| · | third parties provide their services to us on a timely and effective basis; |
| · | we are able to maintain our required supply of raw materials, including krill oil; |
| · | we are able to scale-up production of CaPre with third-party manufacturers to support commercial demand; |
| · | we are able to successfully build a commercial organization, launch CaPre in the United States, and compete in the United States market; |
| · | we are able to secure distribution arrangements for CaPre outside of the US, if it reaches commercialization; |
| · | we are able to manage our future growth effectively; |
| · | we are able to gain acceptance of CaPre in its markets and we are able to serve those markets; |
| · | our patent portfolio is sufficient and valid; |
| · | we are able to secure and defend our intellectual property rights and to avoid infringing upon the intellectual property rights of third parties; |
| 3 |
| · | we are able to take advantage of business opportunities in the pharmaceutical industry; |
| · | we are able to execute on strategic partnerships according to our business plan; |
| · | we are able to continue as a going concern; |
| · | there is no significant increase in competition for CaPre from other companies in the pharmaceutical, medical food and natural health product industries; |
| · | CaPre would be viewed favorably by payers at launch and receive appropriate healthcare reimbursement; |
| · | market data and reports reviewed by us are accurate; |
| · | there are no adverse changes in relevant laws or regulations; and |
| · | we face no product liability lawsuits and other proceedings or any such matters, if they arise, are satisfactorily resolved. |
In addition, the forward-looking information in this MD&A is subject to a number of known and unknown risks, uncertainties and other factors, including those described in this MD&A under the heading “Risk Factors”, many of which are beyond our control, that could cause our actual results and developments to differ materially from those that are disclosed in or implied by the forward-looking information, including, among others:
| · | risks related to timing and possible difficulties, delays or failures in our ongoing TRILOGY Phase 3 program for CaPre; |
| · | nonclinical and clinical trials may be more costly or take longer to complete than anticipated, and may never be completed, or may not generate results that warrant future clinical trials, clinical development and/or commercialization of CaPre; |
| · | our TRILOGY Phase 3 program may not achieve all or any of its primary and secondary endpoints; |
| · | our investigations into the unusually large placebo effect seen in our triglyceride topline data in our TRILOGY 1 clinical trial may not produce any meaningful explanations that could be supported by the FDA; |
| · | based on the final TRILOGY 1 and TRILOGY 2 data, the FDA may require that we conduct additional clinical work to support an NDA for CaPre; |
| · | our anticipated studies and submissions to the FDA may not occur as currently anticipated, or at all; |
| · | the FDA could reject our 505(b)(2) regulatory pathway and/or our NDA; |
| · | while the REDUCE-IT results (a Cardiovascular outcome study conducted by Amarin with their OM3 drug VASCEPA) were positive, on January 13, 2020 AstraZeneca announced that its cardiovascular Phase 3 STRENGTH trial for its OM3 drug EPANOVA had been discontinued due to its low likelihood of demonstrating a benefit to patients with mixed dyslipidaemia (MDL). The potential impacts of the discontinuance of the STRENGTH trial on Acasti’s business and the OM3 drug market in general are not yet known; |
| · | we may encounter difficulties, delays or failures in obtaining regulatory approvals for the initiation of clinical trials or to market CaPre, or the FDA may refuse to approve CaPre, or place restrictions on our ability to commercialize CaPre; |
| · | the FDA may require, or for competitive reasons we may need to conduct additional future clinical trials for CaPre, the occurrence and success of which cannot be assured; |
| · | CaPre may have unknown side effects, or may not prove to be as safe and effective or as potent as we currently believe; |
| · | the FDA may refuse to approve CaPre, or place restrictions on our ability to commercialize CaPre; |
| · | CaPre could be subject to extensive post-market obligations and continued regulatory review, which may result in significant additional expense and affect sales, marketing and profitability; |
| 4 |
| · | we may fail to achieve our publicly announced milestones on time; |
| · | we may encounter difficulties in completing the development and commercialization of CaPre; |
| · | third parties we will rely upon to conduct our TRILOGY Phase 3 program for CaPre may not effectively fulfill their obligations to us, including complying with protocol or FDA requirements; |
| · | there may be difficulties, delays, or failures in obtaining health care reimbursements for CaPre; |
| · | recently enacted and future laws may increase the difficulty and cost for us to obtain marketing approval of and commercialize CaPre and affect the prices we can charge; |
| · | new laws, regulatory requirements, and the continuing efforts of governmental and third-party payors to contain or reduce the costs of healthcare through various means could adversely affect our business; |
| · | the market opportunity for, and demand and market acceptance of, CaPre may not be as strong as we anticipate; |
| · | third parties that we will rely upon to manufacture, supply and distribute CaPre may not effectively fulfill their obligations to us, including complying with FDA requirements; |
| · | there may not be an adequate supply of raw materials, including krill oil, in sufficient quantities and quality and to produce CaPre under cGMP standards; |
| · | we may not be able to meet applicable regulatory standards for the manufacture of CaPre or scale-up our manufacturing successfully; |
| · | as a development stage corporation, we have limited sales, marketing and distribution personnel and resources; |
| · | our patent applications may not result in issued patents, our issued patents may be circumvented or challenged and ultimately struck down, and we may not be able to successfully protect our trade secrets or other confidential proprietary information; |
| · | we may face claims of infringement of third party intellectual property and other proprietary rights; |
| · | we may face product liability claims and product recalls; |
| · | we may face intense competition from other companies in the pharmaceutical, medical food and natural health product industries; |
| · | we have a history of negative operating cash flow and may never become profitable or be able to sustain profitability; |
| · | we have significant additional future capital needs and may not be able to raise additional financing required to fund further research and development, clinical studies, obtain regulatory approvals, build a commercial organization in the United States, and meet ongoing capital requirements to continue our current operations on commercially acceptable terms or at all; |
| · | we may not be able to successfully compete in the United States market with competitors who are larger and have more resources than we do; |
| · | we may acquire businesses or products or form strategic partnerships in the future that may not be successful; |
| · | we may be unable to secure development and/or distribution partnerships to support the development and commercialization of CaPre outside the United States, provide development capital, or market access; |
| · | we rely on the retention of key management and skilled scientific, manufacturing, regulatory and commercial personnel; and |
| · | general changes in economic and capital market conditions could adversely affect us. |
All of the forward-looking information in this MD&A is qualified by this cautionary statement. There can be no guarantee that the results or developments that we anticipate will be realized or, even if substantially realized, that they will have the consequences or effects on our business, financial condition or results of operations that we anticipate. As a result, you should not place undue reliance on the forward-looking information. Except as required by applicable law, we do not undertake to update or amend any forward-looking information, whether as a result of new information, future events or otherwise. All forward-looking information is made as of the date of this MD&A.
| 5 |
Caution Regarding Non-IFRS Financial Measures
The Corporation uses multiple financial measures for the review of its operating performance. These measures are generally IFRS financial measures, but one adjusted financial measure, Non-IFRS operating loss, is also used to assess its operating performance. This non-IFRS financial measure is directly derived from the Corporation’s financial statements and is presented in a consistent manner. The Corporation uses this measure, in addition to the IFRS financial measures, for the purposes of evaluating its historical and prospective financial performance, as well as its performance relative to competitors and to plan and forecast future periods as well as to make operational and strategic decisions. The Corporation believes that providing this Non-IFRS information to investors, in addition to IFRS measures, allows them to see the Corporation’s results through the eyes of management, and to better understand its historical and future financial performance.
Earnings and other measures adjusted to a basis other than IFRS do not have standardized meanings and are unlikely to be comparable to similar measures used by other companies. Accordingly, they should not be considered in isolation. The Corporation uses Non-IFRS operating loss to measure its performance from one period to the next without the variation caused by certain adjustments that could potentially distort the analysis of trends in its operating performance, and because the Corporation believes it provides meaningful information on the Corporation’s financial condition and operating results. Acasti’s method for calculating Non-IFRS operating loss may differ from that used by other corporations.
Acasti calculates its Non-IFRS operating loss measurement by adding to net loss its finance expenses, which includes change in fair value of derivative warrant liabilities and foreign exchange gain (loss), depreciation and amortization, impairment loss, litigation settlement that was settled via the issuance of common shares, and stock-based compensation and by subtracting finance income and deferred tax recovery. Items that do not impact core operating performance of the Corporation are excluded from the calculation as they may vary significantly from one period to another. Acasti also excludes the effects of certain non-monetary transactions recorded, such as stock-based compensation and litigation settlement that was settled via the issuance common shares, from its Non-IFRS operating loss calculation. Excluding this item does not imply it is necessarily non-recurring.
A reconciliation of net loss to Non-IFRS operating loss is presented later in this MD&A.
| 6 |
BUSINESS OVERVIEW
Our Business
We are a biopharmaceutical innovator focused on the research, development and commercialization of prescription drugs using omega-3 fatty acids, or OM3, delivered both as free fatty acids and bound-to-phospholipid esters, or PLs, derived from krill oil. OM3 fatty acids have extensive clinical evidence of safety and efficacy in lowering triglycerides, or TGs, in patients with hypertriglyceridemia, or HTG. Our lead product candidate is CaPre, an OM3 phospholipid therapeutic, which we are developing initially for the treatment of severe HTG, a condition characterized by very high or severe levels of TGs in the bloodstream (≥ 500 mg/dL). In accordance with a study published in 2009 in the Archives of Internal Medicine by Ford et al., it is estimated that three to four million people in the United States have severe HTG. In primary qualitative market research studies commissioned by Acasti in August 2016 and November of 2017 by DP Analytics, a division of Destum Partners, Key Opinion Leaders (KOLs), High Volume Prescribers (HVPs) and Pharmacy Benefit Managers who were interviewed indicated a significant unmet medical need exists for an effective, safe and well-absorbing OM3 therapeutic that can also demonstrate a positive impact on the major blood lipids associated with cardiovascular disease, or CVD, risk. We believe that CaPre may address this unmet medical need, if our Phase 3 clinical program is successful in reproducing what we observed in our Phase 2 data – see “Our TRILOGY Phase 3 Program” further below in this MD&A.
We also believe the potential exists to expand CaPre’s initial indication to the roughly 36 million patients with high TGs in the mild to moderate range (e.g., blood levels between 200 - 499 mg/dL), although at least one additional clinical trial would likely be required to support FDA approval of a Supplemental New Drug Application (SNDA) to expand CaPre’s indication to this segment. Data from our Phase 2 studies indicated that CaPre may have a positive effect in diabetes and other inflammatory and cardiometabolic diseases; consequently, we may also seek to identify new potential indications for CaPre that may be appropriate for future studies and pipeline expansion. In addition, we may also seek to in-license other cardiometabolic drug candidates for drug development and commercialization.
In four clinical trials conducted to date, we saw the following consistent results with CaPre, and we are seeking to demonstrate similar safety and efficacy in our TRILOGY Phase 3 program:
| · | significant reduction of TGs and non-high density lipoprotein cholesterol (non-HDL-C) levels in the blood of patients with mild to severe HTG; | |
| · | no deleterious effect on low-density lipoprotein cholesterol (LDL-C), or “bad” cholesterol, with the potential to reduce LDL-C; | |
| · | potential to increase high-density lipoprotein cholesterol (HDL-C), or “good” cholesterol; | |
| · | potential to benefit diabetes patients by decreasing hemoglobin A1c (HbA1c), a marker of glucose control; | |
| · | good bioavailability (absorption by the body), even under fasting conditions; | |
| · | no significant food effect when taken with either low-fat or high-fat meals; and | |
| · | an overall safety profile similar to that demonstrated by currently marketed OM3s. |
We believe that if we are able to reproduce these results in our TRILOGY Phase 3 program, that this could potentially set CaPre apart from current FDA-approved fish oil-derived OM3 treatment options, and it could give us a significant clinical and marketing advantage.
| 7 |
About Hypertriglyceridemia (HTG)
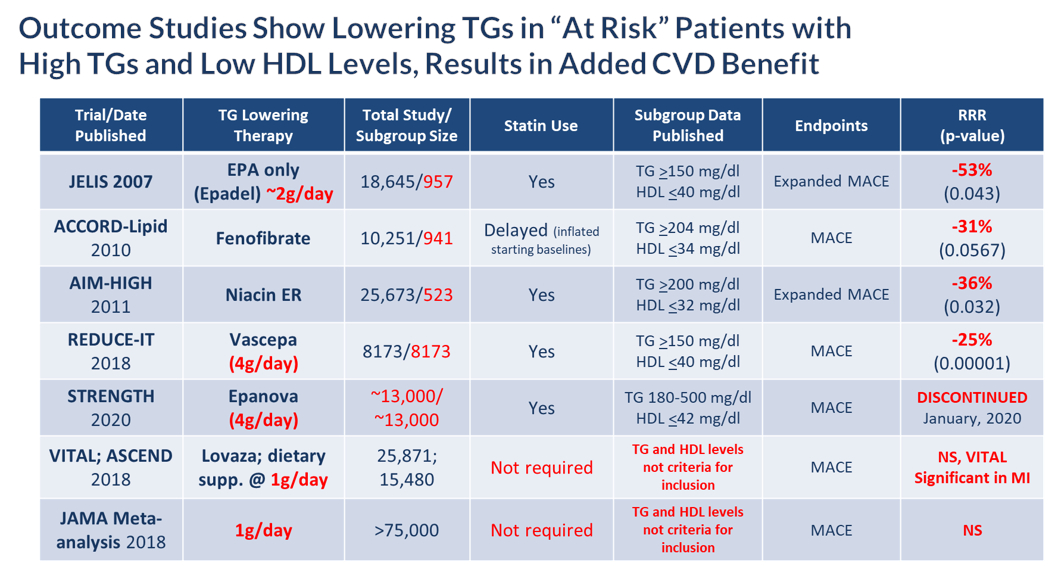
According to the American Heart Association Scientific Statement on Triglycerides and Cardiovascular Disease from 2011, TG levels provide important information as a marker associated with the risk for heart disease and stroke, especially when an individual also has low levels of HDL-C and elevated levels of LDL-C. HTG can be caused by both genetic and environmental factors, including obesity, sedentary lifestyle and high-fat diets. HTG is also associated with comorbid conditions such as chronic renal failure, pancreatitis, nephrotic syndrome, and diabetes. Multiple epidemiological, clinical, genetic studies suggest that patients with elevated TG levels (≥ 200 mg/dL) are at a greater risk of coronary artery disease, or CAD, and pancreatitis, a life-threatening condition, as compared to those with normal TG levels. The genes regulating TGs and LDL-C are equally strong predictors of CAD. Other studies suggest that lowering and managing TG levels may reduce these risks. In addition, the Japan EPA Lipid Intervention Study, or JELIS, demonstrated the long-term benefit of an OM3 eicosapentaenoic acid, or EPA, in preventing major coronary events in hypercholesterolemic patients receiving statin treatment. JELIS found a 19% relative risk reduction in major coronary events in patients with relatively normal TGs but a more pronounced 53% reduction in the subgroup of patients with TGs > 150mg/dL and HDL-C < 40mg/dL. Recently published meta-analyses by Alexander et al. (Mayo Clinic Proceedings, 2017) and Maki et al. (Journal of Clinical Lipidology, 2016) suggest that EPA and docosahexaenoic acid, or DHA, may be associated with reducing coronary heart disease risk to a greater extent in populations with elevated TG levels, and that drugs lowering TG and TG-rich lipoproteins may reduce cardiovascular event risk in patients with elevated TG levels, particularly if associated with low HDL-C. More recently in November of 2018, Amarin published the results of their REDUCE-IT cardiovascular outcome trial (CVOT), which showed that a therapeutic dose of VASCEPA at 4 grams per day, taken on top of a statin, reduced residual cardiovascular risk by 25%. Based on this data, Amarin is currently seeking an expanded label for VASCEPA that would allow use in patients with mild to moderate HTG (200 – 500mg/dl). The table below lists several CVOT studies done over the last 10 years or so, and supports the current thinking that the right dose of any drug (e.g. OM3, Fibrate or Niacin) that reduces TG levels in at risk patients (e.g. those with elevated TGs and low HDL-C), can significantly reduce their cardiovascular risk.
| 8 |
About CaPre
CaPre is a highly purified, proprietary krill oil-derived mixture containing polyunsaturated fatty acids, or PUFAs, primarily composed of OM3 fatty acids, principally eicosapentaenoic acid, or EPA, and docosahexaenoic acid, or DHA, present as a combination of phospholipid esters and free fatty acids. EPA and DHA are well known to be complementary and beneficial for human health, and according to numerous recent clinical studies, may promote healthy heart, brain and visual function (Kwantes and Grundmann, Journal of Dietary Supplements, 2014), and may also contribute to reducing inflammation and blood levels of TGs (Ulven and Holven, Vascular health and risk management, 2015). Krill is a rich natural source of phospholipids and OM3 fatty acids. The EPA and DHA contained in CaPre are delivered as a combination of OM3s as free fatty acids and OM3s bound to phospholipid esters. Both forms allow these PUFAs to reach the small intestine where they undergo rapid absorption and transformation into complex fat molecules that are required for lipid transport in the bloodstream. We believe that EPA and DHA are more efficiently transported by phospholipids sourced from krill oil than the EPA and DHA contained in fish oil, which are transported either by TGs (as in dietary supplements) or as ethyl esters as in other prescription OM3 drugs (such as LOVAZA and VASCEPA). These OM3 ethyl ester prescription products must undergo additional digestion before they are ready for transport into the bloodstream. The digestion and absorption of OM3 ethyl ester drugs requires a particular enzymatic process that is highly dependent on the fat content of a meal – the higher the fat content, the better the OM3 ethyl ester absorption. High fat content meals are not recommended in patients with HTG. We believe that CaPre’s superior absorption profile could represent a significant clinical advantage, since taking it with a low-fat meal represents a healthier and more realistic regimen for patients with HTG who must follow a restricted low-fat diet. CaPre is intended to be used as a therapy combined with positive lifestyle changes, such as a healthy diet and exercise, and can be administered either alone or with other drug treatment regimens such as fibrates and/or statins (a class of drug used to reduce LDL-C). CaPre is intended to be taken orally once or twice per day in capsule form.
Potential Market for CaPre
We believe a significant opportunity exists for OM3 market expansion because, among other things:
| · | Cardiovascular diseases, or CVD, and stroke are the leading causes of morbidity and mortality in the United States. The burden of CVD and stroke in terms of life-years lost, diminished quality of life, and direct and indirect medical costs also remains enormous. According to the American Heart Association, in 2016, CVD cost the American healthcare system $555 billion. By 2035, the cost is estimated to increase to $1.1 trillion; |
| · | Evidence suggests the potential for OM3s as an adjunct to standard treatment in other cardiometabolic indications, such as diabetes and high blood pressure; |
| · | Subgroup analyses from outcome studies conducted since 2007 such as JELIS, ACCORD-Lipid and AIM-HIGH, have all shown that patients who entered these studies with high TGs (above 150 mg/dl) and low HDL (below 40 mg/dl) and received a TG-lowering medication (either an OM3, fibrate or niacin) saw a relative cardiovascular risk reduction of 31 – 53% by the end of the study when compared to placebo or standard of care; |
| · | In February 2019, following the release of the REDUCE-IT results in September 2018, Cantor Fitzgerald projected that based on their market research, prescriptions for OM3s are expected to grow in 2019 by 100%. The most recent (March 2019) audited prescription data from Symphony Health Analytics indicates that VASCEPA sales in August, 2019 had increased by 101% over August, 2018; and |
| · | Several analysts who cover the HTG segment of the market are now projecting that this market could reach $5 to $10 billion or more in the US alone over the next few years. |
According to the American Heart Association, the prevalence of HTG in the United States and globally correlates to the aging of the population and the increasing incidence of obesity and diabetes. Market participants, including the American Heart Association, have estimated that one-third of adults (approximately 70 million people) in the United States have elevated levels of TGs (TGs >150 mg/dL) (Ford, Archives of Internal Medicine, 2009; 169(6):572-578), including approximately 3 to 4 million people diagnosed with severe HTG (Miller et al. Circulation, 2011 and Maki et al. J. Clan. Lipid, 2012). Moreover, according to Ford, Archives of Internal Medicine in a study conducted between 1999 and 2004, 18% of adults in the United States, corresponding to approximately 40 million people, had elevated TG levels equal to or greater than 200 mg/dl, of which only 3.6% were treated specifically with TG-lowering medication (Ford, Archives of Internal Medicine, 2009; 169(6):572-578; Kapoor and Miller, ACC, 2016, Christian et al. Am. J. Cardiology, 2011). We believe this data indicates there is a large underserved market opportunity for CaPre.
| 9 |
CaPre’s target market in the United States for treatment of HTG was estimated by Symphony Health Analytics Audit data to be approximately US$1.4 billion in 2018, with approximately 4.5 million prescriptions written annually. The total global market for treatment of HTG was estimated by GOED Proprietary Research in 2015 to be approximately US$2.3 billion annually. Currently, all marketed OM3 products are approved by the FDA only for patients with severe HTG. We believe there is the potential to greatly expand the treatable market in the United States to the approximately 50 million people with TGs above 150 mg/dl, given the recent FDA approval of expanded labeling for VASCEPA based on the recent positive REDUCE-IT outcome study results. It is not yet known whether the discontinuance by AstraZeneca of its cardiovascular Phase 3 STRENGTH outcome trial for its OM3 drug EPANOVA (announced on January 13, 2020) will have an adverse effect on the size of this potential treatable market. These CVOT studies were designed to evaluate the long-term benefit of lowering TGs on CVD risk with prescription drugs containing OM3 fatty acids in patients with mild to moderately elevated TGs, low HDL-C, and concurrently taking a statin. Additional clinical trials would likely be required for CaPre to also expand its label claims to this segment.
CaPre currently has two FDA-approved and marketed branded competitors (LOVAZA and VASCEPA). Generic LOVAZA became available on the U.S. market in 2013. In spite of generic options, 2017 audited prescription data from IMS NSP indicates that approximately 70% of OM3 prescriptions were written for branded products (predominantly VASCEPA). According to the most recently available Symphony Health Analytics Audit data from August 2019, the U.S. OM3 market for HTG is valued at more than $1.6 billion. However, the number of prescriptions written for branded OM3s is now increasing significantly since Amarin announced its REDUCE-IT results in late 2018.
We conduct market research at least annually with physicians and payers to monitor market developments, reimbursement and clinical practice. Except as otherwise indicated, all of the information that follows under this section has been derived from secondary sources, including audited U.S. prescribing data, and from qualitative U.S. primary market research with physicians and payers conducted for us by DP Analytics, a division of Destum Partners, Inc., or Destum, and more recently by Medical Marketing Economics (MME).
Destum utilized secondary market data and reports to develop market projections for us, and they also conducted primary qualitative market research with physicians and third-party payers, such as PBMs. One-on-one in-depth phone interviews conducted in November 2017 lasting on average 30-60 minutes were conducted with 22 physicians and 5 PBMs. Key insights and data were collected by Destum on current clinical practice for treating patients with HTG, and physician and payer perceptions of the current unmet medical and key economic needs in this space. All interviews were conducted by the same individual at Destum to ensure consistency in the collection of key information. Destum utilized OM3 prescription data from 2009 to 2017 to estimate the size of CaPre’s potential market. Based on discussions with the PBMs, Destum also assumed CaPre would be viewed favorably by payers at launch (e.g., Tier 2 or 3, depending on payer plan, which is comparable to LOVAZA and VASCEPA), provided CaPre is similarly priced. Upon completing the screening questionnaire and being approved for inclusion in Destum’s study, key opinion leaders (KOLs) and high volume prescribers (HVPs), were provided with a study questionnaire and were asked to comment on a target profile for a potential new OM3 “Product X” delivering a “trifecta” of cardio-metabolic benefits similar to the potential efficacy and safety benefits demonstrated by CaPre in our two Phase 1 pharmacokinetic studies and two Phase 2 clinical trials, which we refer to as the Target Product Profile. Respondents were told that the unidentified product was being prepared for a Phase 3 program designed to confirm with statistical significance the product’s safety and efficacy in patients with severe HTG. The Target Product Profile was used by Destum strictly for market research analysis purposes and should not be construed as an indication of future performance of CaPre and should not be read as an expectation or guarantee of future performance or results of CaPre, and will not necessarily be an accurate indication of whether or not such results will be achieved by CaPre in our Phase 3 program.
In the market research conducted for us, KOLs and HVPs interviewed by Destum were asked to assess the level of unmet medical need associated with treating patients with severe HTG based on currently available treatment options. 91% of physicians interviewed by Destum in 2016 indicated that they believe that the current unmet medical need for treating HTG was moderate to high. That number increased to 100% in the subsequent December 2017 research. The reasons identified by these physicians for their dissatisfaction with the currently available OM3s included insufficient lowering of TGs (a complaint principally related to VASCEPA), negative LDL-C effects (a complaint principally related to LOVAZA), the “food effect” or reduced absorption of both LOVAZA and VASCEPA when taken with a low-fat meal (or the corollary to this concern which is that their patients had to take either drug with a fatty meal to get full efficacy benefit), gastrointestinal side effects, and the fishy taste from these fish oil-derived OM3s. Physicians reported that their patients have difficulty swallowing the large 1 gram softgel capsules of VASCEPA and LOVAZA, and they worried about these issues contributing to patient non-compliance. Despite the availability of other drug classes to treat severe HTG, interviewed physicians indicated that they would welcome the introduction of new and improved OM3 products, particularly if they can address these perceived deficiencies.
| 10 |
Interviewed physicians responded favorably to the blinded Target Product Profile of CaPre in the Destum Market Research studies. In the most recent study conducted in December 2017, they indicated that they would prescribe a new OM3 drug with the Target Product Profile to approximately 82% of their patients in the severe HTG patient population and 68% of their patients in the high HTG segment within two years of the new OM3 drug’s approval. Approximately 60% of the interviewed physicians indicated that they would switch to a drug with the Target Product Profile primarily due to the “trifecta effect” of reducing TGs and LDL-C while elevating HDL-C, and the remaining 40% indicated they would switch primarily due to a drug with the Target Product Profile due to the effective reduction of TGs alone. In connection with their responses, the interviewed physicians were instructed to assume the drug with the Target Product Profile and all currently available OM3 products were priced similarly and not subject to any reimbursement or coverage hurdles (e.g., all products were on an equal health care coverage playing field). This assumption was subsequently supported by our interviews with leading PBMs in the United States.
This market research was updated in March 2019 to reflect the more current views of physicians and third party payers following the publication of the REDUCE-IT study results. This updated primary qualitative market research project was conducted by Medical Marketing Economics, and the design of the study was similar to the Destum project, with one-on-one interviews lasting approximately 60 minutes in duration. These interviews were conducted with 10 physicians and 20 pharmacy directors, covering 179,913,005 commercial lives across the United States, consistent with the current payer mix for the OM3 market. CaPre was evaluated positively by physicians with particular value placed on its potential to lower TGs, LDL-C, and HbA1c (this was seen as unique, and especially valued), and to increase HDL-C, as well as its potentially superior tolerability features (e.g. easier to swallow when compared to the ethyl ester fish oils, and no fishy taste or "burpiness"). Importantly, since this research was conducted after the REDUCE-IT trial outcome results, the lack of clinical outcomes data for CaPre at launch was generally not seen as problematic for the majority of the physicians interviewed. On average, physicians indicated that they would begin prescribing CaPre 3 months after launch and would evaluate its performance in their initial patients after 3 to 6 months of use. Depending on favorable experience in initial use, some physicians indicated peak use could begin as quickly as 12 to 18 months after launch. Physicians expect CaPre to be priced similar to VASCEPA, and to have an out-of-pocket cost of approximately $10-$50. Payers also viewed CaPre favorably and did not anticipate any major reimbursement restrictions, with likely coverage at Tier 2 or 3 depending on the payer plan.
Based on both primary market research with pharmacy benefit managers, or PBMs, and audited prescription reports, the pricing for branded products currently averages between US$299 and US$355 per month. Amarin has raised prices for VASCEPA annually since its launch in late 2013. PBMs offer “Preferred Brand” status (Tier 2 or Tier 3), without significant restrictions (i.e., no prior authorization, step edits, or high co-payments) for these branded OM3s. By the end of 2018, VASCEPA had reached about 45% market share in the United States, in spite of generic competition from LOVAZA. Amarin continues to gain market share in the United States and, as of August 2019, had reached more than 50% of the market share based on units. This growth is principally coming from market expansion along with some erosion of generic sales.
We plan to continue to regularly conduct additional market research with KOLs, HVPs, primary care physicians and payers to further develop and refine our understanding of the potential market for CaPre ahead of commercial launch in the United States.
Our Nonclinical Research
In addition to our Phase 2 clinical trials, we carried out an extensive nonclinical program to demonstrate the safety of CaPre in a defined set of studies required by the FDA. These studies were carried out by contract research organizations in compliance with Good Laboratory Practices (GLPs) and conducted on various species of animals recommended by the FDA to investigate the long-term effects of CaPre at doses of up to 65 grams of human equivalent dose over 39 weeks. In these studies, hematological, biochemical, coagulation and overall health parameters of CaPre were evaluated and no toxic effects were observed in any of the segments of the studies. Other studies focused on the potential toxic effects of CaPre on vital systems, such as the cardiovascular, respiratory and central nervous system as evaluated by behavioral studies of the various species. These studies showed that CaPre did not have any adverse or toxic effects on any of the vital systems investigated, again up to doses well above the recommended clinical dose of CaPre. To rule out short term toxic effects of CaPre on genes, genomic toxicity studies were undertaken on accepted cellular and animal models. These studies showed no toxic effects of CaPre on any of the genetic markers indicative of potential gene altering toxic effects.
We believe the studies conducted to date indicate that CaPre is well-tolerated and shows no toxic effects on any of the physiological and vital systems of the tested animals or their genes at doses well above CaPre’s anticipated clinical therapeutic dose of 4 grams daily.
| 11 |
In parallel to our TRILOGY Phase 3 program, we also conducted additional nonclinical studies, including a pre- and postnatal development study in rodents and a 26-week oral carcinogenicity study in transgenic homozygous rasH2 mice. Both study protocols were designed to support an NDA filing for CaPre and were pre-approved by the FDA by means of Special Protocol Assessment (SPA) through the FDA’s Executive Carcinogenicity Assessment Committee. Both studies have now been completed and there was no evidence of a carcinogenic potential of NKPL66 in the transgenic Hemizygous rasH2 mice following daily oral gavage at doses up to 2000 mg/kg/day. In addition, administration of NKPL66 once daily oral gavage was well tolerated in F0 female rats with no evidence of maternal toxicity and no effects on maternal performance. In addition, there were no effects on the development of F1 generation.
Our Clinical Data
CaPre is being developed for the treatment of patients with severe HTG. In two Phase 2 clinical trials conducted by us in Canada (our COLT and TRIFECTA trials), CaPre was well-tolerated at all doses tested, with no serious adverse events that were considered treatment-related. Among the reported adverse events with an occurrence of greater than 2% of subjects and greater than placebo, only diarrhea had an incidence of 2.2%.
In both Phase 2 clinical trials, CaPre significantly lowered TGs in patients with mild to severe HTG. Importantly, in these studies, CaPre also demonstrated no deleterious effect on LDL-C (unlike LOVAZA and EPANOVA, which had been shown to significantly increase LDL-C in patients with severe HTG). Further, our Phase 2 data indicated that unlike LOVAZA, CaPre may actually reduce LDL-C with a 4 gram per day dose (a dose equivalent to VASCEPA and LOVAZA). LDL-C is undesirable because it accumulates in the walls of blood vessels, where it can cause blockages (atherosclerosis). Clinically, the phospholipids may potentially not only improve the absorption, distribution, and metabolism of omega-3s, but they may also decrease the synthesis of LDL cholesterol in the liver, impede or block cholesterol absorption, and stimulate lipid secretion from bile. In the Phase 2 trials, CaPre also significantly reduced non-HDL-C (all cholesterol contained in the bloodstream except HDL-C), which is also considered to be a marker of cardiovascular disease. The COLT trial data showed a mean increase of 7.7% in HDL-C with CaPre at 4 grams per day (p=0.07). Further analysis of the data from our on-going TRILOGY Phase 3 program will be required to demonstrate CaPre’s statistical significance with respect to lowering LDL-C and increasing HDL-C. Finally, we saw a statistically significant reduction of HbA1c in the CaPre 4g treatment group in the COLT study after only 8 weeks on drug in a diabetic population of patients with HbA1c levels at or below 7.0% at baseline. This interesting and potentially differentiating effect is being investigated more thoroughly in our TRILOGY Phase 3 program, where a larger proportion of the patients are diabetic, with HbA1c levels up to 9.5%, and they will be followed for 6 months.
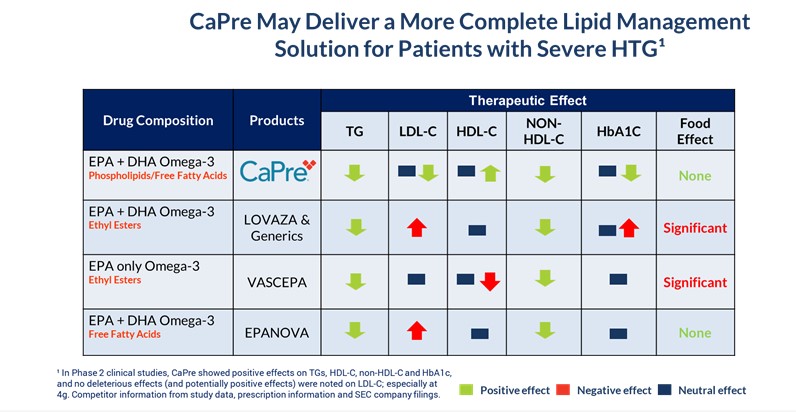
We believe that these multiple potential cardiometabolic benefits, if confirmed in our on-going TRILOGY Phase 3 program, could be significant differentiators for CaPre in the marketplace, as no currently approved OM3 drug has shown an ability to positively modulate all four of these important blood lipids (TGs, non-HDL-C, LDL-C and HDL-C) in the treatment of patients with dyslipidemia. We also believe that if supported by additional clinical trials, CaPre has the potential to become the best-in-class OM3 compound for the treatment of mild to moderate HTG.
In summary, in addition to effectively reducing TG levels in patients with mild to severe HTG, clinical data collected by us to date indicates that CaPre may also have:
| · | beneficial clinical effects on other blood lipids, such as HDL-C (good cholesterol) and non-HDL-C; | |
| · | no deleterious effect on, and may potentially reduce, LDL-C (bad cholesterol) levels; | |
| · | potential to benefit diabetes patients by reducing HbA1c, an important marker of diabetes; and | |
| · | absorption capability that, unlike VASCEPA and LOVAZA, is not meaningfully affected by the fat content of a meal consumed prior to drug administration, providing patients with the reassurance that following their physician-recommended low-fat diet will still result in high absorption. |
We believe that these features could set CaPre apart from currently available FDA-approved OM3 treatment options in the marketplace and could give us a significant clinical and marketing advantage.
CaPre’s potential clinical benefits as compared to currently available FDA-approved OM3 treatment options are summarized in the table below and indicate that CaPre may deliver a more complete lipid management solution for patients with severe HTG:
| 12 |
| 13 |
Our TRILOGY Phase 3 Program
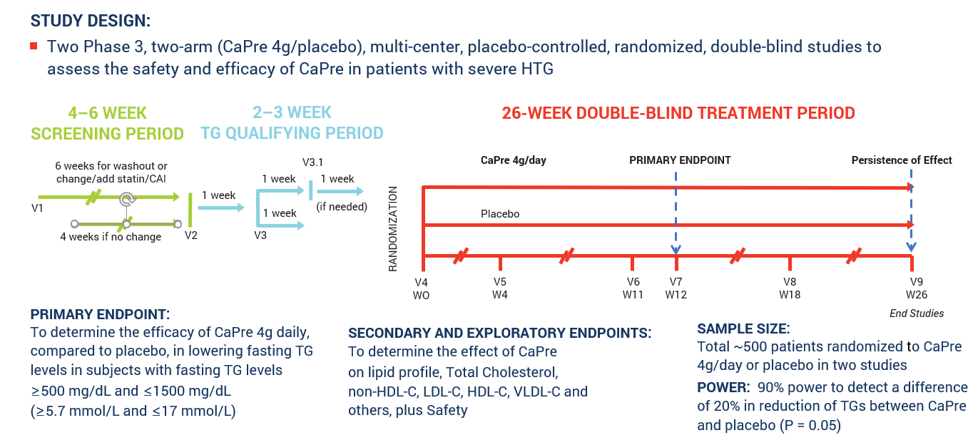
In March 2017, we announced our plans to proceed with our TRILOGY Phase 3 program following our End-of-Phase 2 meeting with the FDA in February 2017. Based on the guidance we received from the FDA, we implemented two pivotal, randomized, placebo-controlled, double-blinded Phase 3 studies to evaluate the safety and efficacy of CaPre in patients with severe HTG. These studies of 26-week duration will evaluate CaPre’s ability to lower TGs from baseline in approximately 500 patients (approximately 250 per study) randomized to either 4 grams daily or placebo. The FDA’s feedback supported our plan to conduct two studies in parallel, potentially reducing the cost and shortening the time to an NDA submission. These studies were conducted in 125 sites across North America.
The primary endpoint of these studies is to determine the efficacy of CaPre at 4 grams/day compared to placebo in lowering TGs after 12 weeks in severe HTG patients, and to confirm safety and persistence of TG lowering effect by continuing to follow these patients for the full 26 weeks. The study was designed to provide at least 90% statistical power to detect a difference of at least a 20% decrease from baseline in TGs between CaPre and placebo. In addition, the Phase 3 studies included numerous secondary and exploratory endpoints, which are designed to assess the effect of CaPre on the broader lipid profile and certain metabolic, inflammatory and CVD risk markers.
In November 2017, we announced that Dariush Mozaffarian, M.D., Dr.P.H., agreed to serve as the principal investigator of our Phase 3 clinical program. Dr. Mozaffarian is a cardiologist and epidemiologist serving as the Jean Mayer Professor of Nutrition & Medicine, and the Dean of the Friedman School of Nutrition Science & Policy at Tuft’s University. His widely published research focuses on how diets, such as those rich in OM3s, and lifestyle influence cardiometabolic health and how effective policies can improve health and wellness.
Late in 2017, based on feedback from the FDA, we finalized our Chemistry, Manufacturing, and Controls plans and the clinical trial design that supports our TRILOGY Phase 3 program. In parallel with our Phase 3 clinical trial planning, additional current Good Manufacturing Practices (cGMP) production lots of API (known as NKPL66) and CaPre were manufactured, enabling us to build the CaPre and placebo inventory required to support the activated clinical trial sites and complete patient randomization. In the first calendar quarter of 2018, additional lots of CaPre were manufactured for use in our Phase 3 program. Acasti recently entered into a supply agreement with a major manufacturer of raw krill oil (RKO), which we anticipate will secure RKO material sufficient for the first two years of our planned commercial launch.
We initiated our TRILOGY Phase 3 program and began site activation and patient enrollment on schedule at the end of 2017. We are working with a major clinical research organization to manage our TRILOGY Phase 3 program. The TRILOGY studies continued to progress on schedule throughout 2018 and 2019, and as of the end of September 2019, our two Phase 3 TRILOGY trials had reached 100% patient randomization at clinical sites across the United States, Canada, and Mexico.
Our first study, designated as TRILOGY 1, was conducted exclusively in the United States and was fully randomized with a final total of 242 patients. On January 13, 2020 we released topline results for TRILOGY 1, which, despite meaningful TG lowering in the CaPre arm, did not reach statistical significance due to an unusually large placebo effect – see “TRILOGY 1 Topline Results” below in this MD&A. Our second study, designated TRILOGY 2, which is also fully randomized, with a total of 278 patients, and is being conducted in the United States, Canada and Mexico.
| 14 |
The following chart illustrates the design and dosing of our TRILOGY Phase 3 program for CaPre.
TRILOGY Phase 3 Clinical Program
TRILOGY 1 Topline Results
On January 13, 2020 we announced preliminary topline results for the primary endpoint (triglyceride reduction at 12 and 26 weeks) from our Phase 3 TRILOGY 1 trial for CaPre.
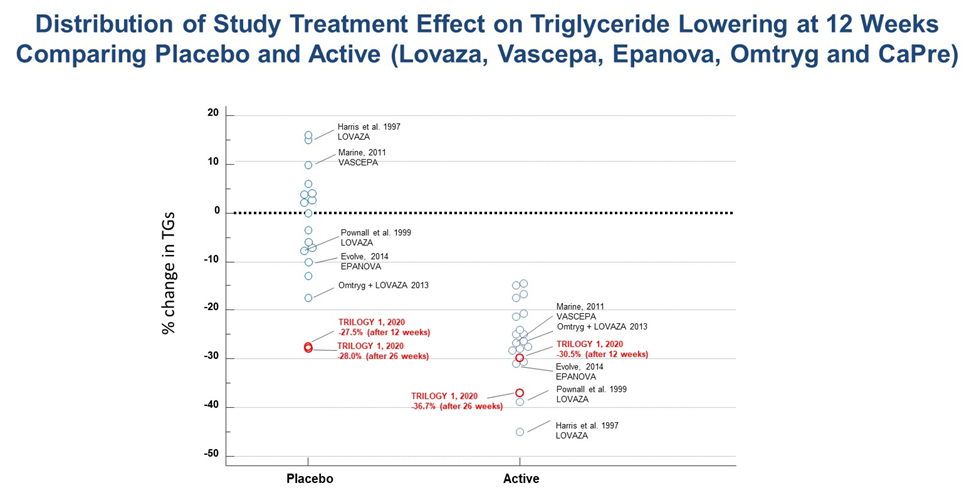
Acasti reported a 30.5% median reduction in triglyceride (TG) levels among all patients receiving CaPre, compared to a 27.5% median reduction in triglyceride levels among patients receiving placebo at 12 weeks. We also reported a 42.2% median reduction in TGs among patients receiving CaPre while on background statin therapy at 12 weeks, compared to a 31.5% median reduction in TG levels among patients receiving placebo and on background statin therapy. In addition, the Company reported a 36.7% median reduction in TG levels among patients receiving CaPre at 26 weeks (end of the study), compared to a 28.0% median reduction in TG levels among patients receiving placebo. Both the placebo and CaPre study groups experienced significant reductions in TGs within the first four weeks from baseline, and even though the difference at 12 and 26 weeks was in favor of CaPre, due to the unexpectedly large placebo response, TRILOGY 1 did not reach statistical significance. The safety profile of CaPre in TRILOGY 1 was similar to placebo, as there was no significant difference in treatment-related serious adverse events in the trial. Results for all of the secondary and exploratory endpoints as well as topline results for TRILOGY 2 have subsequently been delayed subject to our ongoing investigation into the unusually large placebo effect observed in TRILOGY 1.
The observed reductions in TG levels in the placebo group were far greater than that seen in any previous triglyceride lowering trial with a prescription omega-3. The placebo used in the TRILOGY trials is simple cornstarch, which is a complex carbohydrate with a low glycemic index, and consequently would be expected to have a neutral effect on key biomarkers of patients in the placebo group. In similar previously conducted triglyceride lowering trials involving prescription omega-3 preparations, the placebo responses (using corn oil, olive oil, or vegetable oil) ranged from a change of +16% to -17% across 18 interventions arms, with 14 of 18 arms ranging between +10% to -10%. Note that a low fat diet contains around 55% of energy as carbohydrates, and represents around 180-220g of carbohydrates a day. Consequently, an additional 4g/day of cornstarch (representing roughly 2% of daily intake) would not significantly add to this expected daily intake. In addition, cornstarch is generally regarded as safe (G.R.A.S.) and is a commonly used placebo in the pharma industry (the so-called ‘sugar pill’) that is well known to be an inert and inactive excipient, with low nutritive value. This justification was also noted by FDA.
| 15 |
A table summarizing the placebo and active triglyceride lowering results from all of these previous hypertriglyceridemia trials is presented below:
With more investigation, we have noted a highly unusual placebo response in its topline triglyceride reduction primary endpoint, far greater than seen in any prior omega-3 triglyceride lowering trials, with 5 sites out of the total 54 enrolling sites disproportionately contributing to this placebo response. These sites accounted for about 36% of the 242 patients enrolled in the TRILOGY 1 study. By comparison, TRILOGY 2 was conducted at 71 sites in Canada, Mexico and the United States that enrolled a total of 278 patients. The 5 sites also participated in TRILOGY 2, however these sites accounted for only 12% of the total patients, with the majority of these patients coming from only 3 sites.
Despite monitoring activities conducted throughout the TRILOGY 1 trial to ensure adherence to the protocol and identify protocol violations, we have subsequently identified some unexpected and inconsistent findings that we believe may have negatively contributed to the overall topline results. These findings are now being further explored via a comprehensive and rigorous review of data and patient medical records by an independent team of auditors. To support this effort, the Company, its independent Clinical Research Organization (CRO) that conducted the TRILOGY studies, its principal investigator Dr. Mozaffarian, and other clinical and regulatory advisors, are conducting a thorough review of all data and records from patients taking both CaPre and placebo. This assessment is well underway, and the Company has also determined that a thorough investigation of the data must be completed and reviewed with the FDA, before the Company can report the findings from TRILOGY 1 and the implications for TRILOGY 2.
| 16 |
Consequently, we intend to request a meeting with the FDA to discuss the TRILOGY 1 data, and will seek their guidance about how to conduct the analysis of the TRILOGY 2 data prior to unblinding TRILOGY 2. The Company continues to remain blinded to the TRILOGY 2 data. Upon submission of the meeting request, which is expected to be sent to the FDA in calendar Q2, 2020, the FDA will have 75 days to review the findings and provide feedback and guidance.
Given the need to complete the audit and review of the TRILOGY 1 data, and obtain FDA feedback, we intend to delay the unblinding of the topline results for TRILOGY 2 until sometime in calendar Q3 of 2020. Acasti will provide further guidance as to the timing of reporting TRILOGY 2 data based on progress of the audits and feedback from the FDA. Accordingly, key secondary and exploratory endpoints from both TRILOGY 1 and TRILOGY 2 studies, would now be expected as soon as possible after the unblinding of TRILOGY 2 results.
If the interpretation of the analyses produced as an outcome of the TRILOGY 1 audits and post-hoc data review are supported by the FDA, and if TRILOGY 2 achieves statistical significance, Acasti believes it may still have a viable path forward to file an NDA for CaPre.
Our Regulatory Strategy for CaPre
Our strategy is to develop CaPre for the treatment of severe HTG. The TRILOGY Phase 3 program was designed to evaluate the clinical effect of CaPre on TGs, non-HDL-C, LDL-C, and HDL-C levels together with a variety of other cardiometabolic biomarkers in patients with severe HTG.
If our TRILOGY Phase 3 program is successful, we intend to pursue a 505(b)(2) regulatory pathway towards an NDA approval in the United States. A 505(b)(2) regulatory pathway is defined in the U.S. Federal Food Drug and Cosmetic Act (FDCA) as an NDA containing investigations of safety and effectiveness that are being relied upon for approval and were not, in whole, conducted by or for the applicant, and for which the applicant has not obtained a right of reference. 505(b)(2) regulatory pathways differ from a typical NDA because they allow a sponsor to rely, at least in part, on the FDA’s findings of safety and/or effectiveness for a previously approved drug. We intend to pursue the 505(b)(2) regulatory pathway as a strategy to leverage the large body of safety data for LOVAZA, which could accelerate and streamline the development of CaPre and reduce associated costs and risks. We are conducting two Phase 3 studies to independently assess CaPre’s effectiveness in lowering TGs, and its broader effect in patients with cardiometabolic disease. Consequently the use of this 505(b)(2) pathway still allows CaPre to retain its New Chemical Entity (NCE) status due to its novel, patented OM3 free fatty acid/phospholipid ester formulation. In connection with our intended use of the 505(b)(2) pathway, the FDA supported our proposal to conduct our Bridging Study that compared CaPre (which has an OM3 free fatty acid/phospholipid composition) with LOVAZA (which has an OM3-acid ethyl esters composition) in healthy volunteers. In February 2017, we met with the FDA at an End-of-Phase 2 meeting where our Bridging Study data was discussed. We confirmed with the FDA the 505(b)(2) regulatory approach to use the safety data for LOVAZA and finalized the study design for our Phase 3 program that would be required for NDA approval.
| 17 |
Our Intellectual Property Strategy
Under a license agreement we entered into with Neptune in August 2008, which was later amended on February 9, 2009 and March 7, 2013 (the “License Agreement”), we received an exclusive license to use certain intellectual property of Neptune (which includes several patents) to develop and commercialize CaPre and our novel and active pharmaceutical ingredients, or APIs, for use in pharmaceutical and medical food applications in the cardiometabolic field. The term of the License Agreement expires on the date of the last-to-expire licensed patents in 2022. As the result of a royalty prepayment transaction we entered into with Neptune on December 4, 2012, we are not required to pay any royalties to Neptune under the License Agreement during its term for the use of the licensed intellectual property.
Upon the expiry of the License Agreement and related patents, we believe that CaPre will be covered under our own issued and pending patents, and we do not believe that we will afterwards require any licenses to support the commercialization of CaPre.
We currently have patents granted and allowed in the following countries: United States, Canada, Russia, Belgium, Switzerland, Germany, Denmark, Spain, Finland, France, United Kingdom, Italy, Netherlands, Norway, Portugal, Sweden, Japan, Israel, Australia, China, Mexico, Panama, Saudi Arabia, Taiwan, South Africa, Chile and South Korea. We continue to expand our own intellectual property, or IP, patent portfolio. We have filed patent applications in more than 20 jurisdictions, including with the European Patent Office (but excluding the individual countries where we have subsequently registered), and in all major countries in North America, Asia and Australia for our “Concentrated Therapeutic Phospholipid Composition”, or Proprietary Composition, to treat HTG. We currently have 20 issued or allowed patents (including registered European countries) and numerous patent applications pending. A patent is generally valid for 20 years from the date of first filing. However, patent terms can be subject to extensions in some jurisdictions in order to compensate, for example, for delays caused by the patent office during prosecution of the patent application or for regulatory delays during the pre-market approval process.
On January 9, 2019, we announced a Certificate for a European Patent had been issued by the European Patent Office. The granted patent is valid until 2030 and relates to a concentrated phospholipid composition and method of using the same for modulating blood lipids. This patent was validated in Belgium, Switzerland, Germany, Denmark, Spain, Finland, France, United Kingdom, Italy, Netherlands, Norway, Portugal and Sweden. We also received notices of allowances for patents in Chile, Mexico and Israel.
We believe these patents and patent applications increase potential commercial opportunities for CaPre, including through possible licensing and partnership opportunities. We are committed to building a global portfolio of patents to ensure long-lasting and comprehensive intellectual property protection and to safeguard potentially valuable market expansion opportunities.
| 18 |
Our patent No. 600167 in New Zealand, which is in force until 2030 and relates to a concentrated phospholipid composition comprising 60% or greater PL concentration and method of using the same for treating cardiovascular diseases, has been opposed by BIO-MER Ltd. The evidentiary stage in the New Zealand patent opposition has been completed. The next step is the hearing. In our view, no new prior art has been presented that was not already considered in other jurisdictions, such as in the United States, where our patents are in force.
We have received a notice issued from the Japan Patent Office (JPO) indicating that a third party filed an opposition against our Japanese Patent No. 6346121. The claim amendment was filed by Acasti and the Corporation was successful in overcoming the prior art cited in the opposition.
Our China divisional application (201410490601.5) with claims covering 50% w/w to 70% w/w of phospholipids was granted. This patent is in the process of being registered in Hong Kong and Macau through a formality process requiring no substantive submission.
The trademark CaPre® is registered in the United States, Canada, Australia, China, Japan and Europe. We are currently in the process of developing a new brand name and logo for CaPre for launch into the U.S. market. That name, once it is developed, will be trademarked in all of the major jurisdictions around the world. In addition, two PCT applications that cover our encapsulation apparatus and manufacturing process have been filed in all territories under the PCT treaty, while maintaining industrial trade secrets and know-how. We are in the process of converting the provisional application covering our starting material composition (RKO) for the use of CaPre manufacturing into a PCT application. On January 10th, 2020, we filed a provisional application to cover other indications of CaPre in inflammatory-related diseases entitled “Composition that promote pro-resolving mediators”.
Our Business and Commercialization Strategy
Key elements of our business and commercialization strategy include initially obtaining regulatory approval for CaPre in the United States for severe HTG. We plan to launch CaPre ourselves in the U.S. market once regulatory approval is obtained. Our preferred strategy outside the United States is to commercialize CaPre through regional or country-specific strategic partnerships, and to potentially seek support and funding from each partner for in-country clinical development, registration and commercialization activities. We believe that a late development-stage and differentiated drug candidate like CaPre could be attractive to various global, regional or specialty pharmaceutical companies, and we are taking a targeted approach to partnering and licensing in various geographies.
Our key commercialization goals include:
| · | complete our TRILOGY Phase 3 program and, assuming the results are ultimately positive, file an NDA to obtain regulatory approval for CaPre in the United States, initially for the treatment of severe HTG, with the potential to afterwards expand CaPre’s indication to the treatment of high TGs (although at least one additional clinical trial would likely be required to expand CaPre’s indication to this segment), and possibly other additional indications; |
| · | continue to strengthen our patent portfolio and other intellectual property rights; |
| · | continue planning for the potential launch of CaPre in the United States; and |
| · | continue to pursue strategic opportunities outside of the United States, such as licensing or similar transactions, joint ventures, partnerships, strategic alliances or alternative financing transactions, to provide development capital, market access and other strategic sources of capital. |
| · | continue to search for additional new assets for in-licensing or acquisition that could be synergistic with CaPre, and leverage our commercial organization. |
| 19 |
We expect that additional time and capital will be required to complete the filing of an NDA to obtain FDA approval for CaPre in the United States, and to complete business development collaborations, marketing and other pre-commercialization activities before reaching the commercial launch of CaPre in the United States.
Recent Developments
| · | On September 9, 2019, Acasti announced that the Corporation was awarded up to $750,000 in non-dilutive and non-repayable funding, as well as technical and business advisory services, from the National Research Council of Canada Industrial Research Assistance Program (NRC IRAP) to apply towards eligible research and development disbursements of the Corporation’s unique commercial production platform for CaPre. |
| · | On September 30, 2019, Acasti announced that 100% of the required total patients for its two Phase 3 studies had been randomized, and nearly 80% of the patients in both studies combined had completed their 6-month plans. |
| · | On September 30, 2019, Acasti made the determination that the Corporation will migrate from reporting in IFRS to US GAAP effective beginning with Q4, FY’20 (March 31, 2020 year-end) reports. |
| · | On November 4, 2019, Acasti announced that it had partnered with Aker BioMarine to deliver raw krill oil (RKO) to Acasti, under a two-year, fixed price supply agreement. |
| · | On November 7, 2019, Acasti announced the publication of a CaPre pharmacokinetics study entitled, “Evaluation of OM3-PL/FFA Pharmacokinetics After Single and Multiple Oral Doses in Healthy Volunteers” in a leading peer-reviewed journal, Clinical Therapeutics. The study showed that the bioavailability of CaPre did not appear to be meaningfully affected by the fat content of the meal consumed before dose administration. |
| · | On November 18, 2019, Acasti released preliminary new animal study data which provides additional insights into CaPre’s potential mechanism of action in diabetes. The preliminary findings obtained for the diabetes mouse study showed that CaPre may promote insulin secretion as seen by statistically significant results produced in a standard glucose challenge test, thus suggesting a mechanism of action different and unique when compared to metformin, which does not promote insulin secretion. |
| · | On November 26, 2019, Acasti announced that the last patient completed their final visit in the Corporation's TRILOGY 1 Phase 3 trial of CaPre. |
| · | On December 23, 2019, Acasti provided an update on the expected delay of topline results into January 2020 for the Corporation's TRILOGY 1 Phase 3 trial of CaPre. The delay was caused by gaps in the data when the dataset was transferred from the Central laboratory to the CRO data management group. When this problem was identified by the CRO data management group, it triggered an immediate hold on the data transfer to the CRO statistical group and initiated a full quality review by the CRO of the processes and procedures involved at the central testing laboratory. This review was completed in early January 2020, and topline results for TRILOGY 1 were subsequently released on January 13, 2020. A more comprehensive audit of the central laboratory is currently ongoing. |
| · | On December 18, 2019, Acasti incorporated a new wholly owned subsidiary named Acasti Innovation AG (“AIAG”) under the laws of Switzerland for the purpose of future development of the Corporation’s intellectual property and global distribution of its products. AIAG currently does not have any operations. |
| · | On January 9, 2020, Acasti announced that the last patient completed their final visit in Acasti's TRILOGY 2 Phase 3 trial of CaPre. |
| · | On January 13, 2020, Acasti reported topline results for TRILOGY 1, which, despite showing a meaningful reduction of TGs in the CaPre arm, did not reach statistical significance due to an unusually large placebo effect. |
| · | On February 10, 2020, Acasti provided an update on its TRILOGY 1 and TRILOGY 2 Phase 3 Trials of CaPre. This announcement disclosed that a full investigation was being conducted, including specific site audits, and a full audit of the central testing laboratory involved its TRILOGY 1 Phase 3 trial for CaPre. It also announced that once the full analysis of TRILOGY 1 is completed, that the Company would request a meeting with the FDA to discuss the data and seek guidance on how to modify the statistical analysis plan (SAP) for TRILOGY 2 before unblinding the results. This important decision will push out the reporting of TRILOGY 2 results until calendar Q3 of 2020. |
| 20 |
Basis of presentation of the financial statements
The Corporation is subject to a number of risks associated with its ongoing priorities, including the completion of the clinical program for CaPre and its results, the filing and approval of an NDA, the establishment of strategic alliances and the development of new pharmaceutical products and their marketing. The Corporation’s current product in development requires approval from the U.S Food and Drug Administration and equivalent regulatory organizations in other countries before sale can be authorized. Certain risks have been reduced for the longer term with the outcome of the Corporation’s actions, including the scale up of manufacturing of CaPre to 20 tons to support commercial launch, expansion of market development activities, and its intellectual property strategy execution with filed patent applications in more than 20 jurisdictions, with 20 issued patents and with numerous additional patent applications pending. Certain other risks remain such as a successful outcome for TRILOGY and ability to file an NDA and receive FDA approval. The Corporation has incurred significant operating losses and negative cash flows from operations since inception. To date, the Corporation has financed its operations through the public offering and private placement of Common Shares, (“Common Shares”; with or without warrants) and convertible debt, the proceeds from research grants and research tax credits, and the exercises of warrants, rights and options. To achieve the objectives of its business plan, Acasti plans to raise the necessary funds through a possible combination of additional warrant exercises, debt facilities, securities offerings and the establishment of strategic alliances, as well as additional research grants and research tax credits. The ability of the Corporation to complete needed financing and ultimately achieve profitable operations is dependent on a number of factors outside of the Corporation’s control. See “Risk Factors” in this MD&A and in Acasti’s Annual Report on Form 20-F for the fiscal year ended March 31, 2019
The Corporation has incurred operating losses and negative cash flows from operations since inception. The Corporation’s current assets of $29.6 million as at December 31, 2019 include cash and cash equivalents and marketable securities totaling $25.7 million. The Corporation’s current liabilities total $14.3 million at December 31, 2019 and are comprised primarily of amounts due to or accrued for creditors. Management projects that additional funds will be needed in the future, for activities necessary to prepare for commercial launch, including the scale up of our manufacturing operations, the completion of the potential regulatory (NDA) submission package (assuming positive Phase 3 clinical results), and the expansion of business development and US commercial launch activities. The Corporation is working towards development of strategic partner relationships, as well as actively seeking additional non-dilutive funds in the near future, but there can be no assurance as to when or whether Acasti will complete any strategic collaborations or non-dilutive financings. Consequently, the Corporation may need to raise additional equity capital in the future to fund these activities. In particular, raising additional capital is subject to market conditions not within the Corporation’s control. If the Corporation does not raise additional funds or find one or more strategic partners, it may not be able to realize its assets and discharge its liabilities in the normal course of business. As a result, there exists a material uncertainty that casts substantial doubt about the Corporation’s ability to continue as a going concern and, therefore, realize its assets and discharge its liabilities in the normal course of business.
The consolidated financial statements have been prepared on a going concern basis, which assumes the Corporation will continue its operations in the foreseeable future and will be able to realize its assets and discharge its liabilities and commitments in the ordinary course of business. These consolidated financial statements do not include any adjustments to the carrying values and classification of assets and liabilities and reported expenses that may be necessary if the going concern basis was not appropriate for these financial statements. If the Corporation was unable to continue as a going concern, material write-downs to the carrying values of the Corporation’s assets, including the intangible asset, could be required.
| 21 |
SELECTED FINANCIAL INFORMATION
| Three-month periods ended | Nine-month periods ended | |||||||||||||||
| December 31, 2019 | December 31, 2018 | December 31, 2019 | December 31, 2018 | |||||||||||||
| $ | $ | $ | $ | |||||||||||||
| Net loss | (15,728 | ) | (4,610 | ) | (55,827 | ) | (34,760 | ) | ||||||||
| Basic and diluted loss per share | (0.18 | ) | (0.07 | ) | (0.67 | ) | (0.75 | ) | ||||||||
| Non-IFRS operating loss1 | (6,520 | ) | (9,651 | ) | (22,809 | ) | (28,062 | ) | ||||||||
| Total assets | 38,879 | 59,658 | 38,879 | 59,658 | ||||||||||||
| Working capital2 | 15,309 | 33,881 | 15,309 | 33,881 | ||||||||||||
| Total non-current financial liabilities | 30,758 | 15,181 | 30,758 | 15,181 | ||||||||||||
| Total equity | (6,180 | ) | 30,624 | (6,180 | ) | 30,624 | ||||||||||
RECONCILIATION OF NET LOSS TO NON-IFRS OPERATING LOSS
| Three-month periods ended | Nine-month periods ended | |||||||||||||||
| December 31, 2019 | December 31, 2018 | December 31, 2019 | December 31, 2018 | |||||||||||||
| $ | $ | $ | $ | |||||||||||||
| Net loss | (15,728 | ) | (4,610 | ) | (55,827 | ) | (34,760 | ) | ||||||||
| Add (deduct): | ||||||||||||||||
| Stock-based compensation | 609 | 336 | 2,232 | 913 | ||||||||||||
| Depreciation and amortization | 726 | 723 | 2,099 | 2,096 | ||||||||||||
| Financial expenses | 7,873 | (6,100 | ) | 28,687 | 3,689 | |||||||||||
| Non-IFRS operating loss | (6,520 | ) | (9,651 | ) | (22,809 | ) | (28,062 | ) | ||||||||
COMMENTS ON THE SIGNIFICANT VARIATIONS OF RESULTS FROM OPERATIONS FOR THE THREE AND NINE-MONTH PERIODS ENDED DECEMBER 31, 2019 AND 2018
The net loss of $15,728 or ($0.18) per share for the three months ended December 31, 2019 increased by $11,118 from the net loss $ 4,610 for the three months ended December 31, 2018, while the loss per share increased by ($0.11) per share from the loss of ($0.07) per share loss for the three months ended December 31, 2018. The per share loss increased due to the higher net loss partially offset by the issuance of 10.9 million shares in relation mainly to the exercise of warrants from July to December 2019 and the sale of shares under the at-the-market program during November and December 2019.
The increased net loss resulted primarily from a net financial expenses of $7,873 for the three months ended December 31, 2019, as compared to net financial income of $6,100 for the three months ended December 31, 2018, due mostly to the change in fair value of the warrant derivative liability partially offset by a decrease in the number of warrants. In addition, the increase in net loss is the result of increased sales and marketing headcount to support expanded business and development activities, and of additional administrative fees incurred in connection with the implementation of a new Enterprise Resource Planning (“ERP”) system, increased insurance costs, as well as increased accounting and legal fees. Furthermore, stock-based compensation expense increased by $273 as result of new grants. The increase in administrative and sales and marketing expenses were offset by a decrease on research and development expenses as the Phase 3 clinical trial program is getting closer to completion.
The net loss of $55,827 or ($0.67) per share for the nine months ended December 31, 2019 increased by $21,067 from the net loss for the nine months ended December 31, 2018, while the loss per share decreased by ($0.08) per share from the loss of ($0.75) per share loss for the nine months ended December 31, 2018. The per share loss decreased due to the issuance of 63.4 million shares in relation mainly to the public financings that occurred in May and October of 2018, the exercise of warrants during July and August 2019 and the sale of shares under the at-the-market program during November and December 2019.
The increased net loss resulted primarily from a net financial expenses of $28,687 for the nine months ended December 31, 2019, as compared to net financial expenses of $3,689 for the nine months ended December 31, 2018, due mostly to the change in fair value of the warrant derivative liability, partially offset by a decrease in the number of warrants. In addition, the increase in net loss is the result of creating our senior commercial team during the second quarter of fiscal year 2019 and subsequent increase in headcount to support expanded business and development activities, and of additional administrative fees incurred in connection with the implementation of a new ERP system and increased insurance cost, as well as increased accounting and legal fees. Furthermore, stock-based compensation expense increased by $1,319 as result of new grants. The increase in administrative and sales and marketing expenses were offset by a decrease on research and development expenses as the Phase 3 clinical trial program is getting closer to completion.
____________________________
1 The Non-IFRS operating loss is not a standard measure endorsed by IFRS requirements. A reconciliation to the Corporation’s net loss is presented above.
2 Working capital is calculated by subtracting current liabilities from current assets. Because there is no standard method endorsed by IFRS requirements, the results may not be comparable to similar measurements presented by other public companies.
| 22 |
Breakdown of major components of the statement of earnings and comprehensive loss.
| Research and development expenses | ||||||||||||||||
| Three Months Ended | Nine Months Ended | |||||||||||||||
| December 31, 2019 | December 31, 2018 | December 31, 2019 | December 31, 2018 | |||||||||||||
| $ | $ | $ | $ | |||||||||||||
| Salaries and benefits | 592 | 372 | 1,701 | 1,129 | ||||||||||||
| Research contracts | 2,797 | 8,349 | 12,750 | 23,492 | ||||||||||||
| Professional fees | 783 | 50 | 1,321 | 638 | ||||||||||||
| Other | 193 | 98 | 410 | 323 | ||||||||||||
| Government grants & tax credits | (158 | ) | (110 | ) | (258 | ) | (290 | ) | ||||||||
| Sub-total | 4,207 | 8,759 | 15,924 | 25,292 | ||||||||||||
| Stock-based compensation | 136 | 74 | 510 | 183 | ||||||||||||
| Depreciation and amortization | 725 | 723 | 2,099 | 2,096 | ||||||||||||
| Total | 5,068 | 9,556 | 18,533 | 27,571 | ||||||||||||
| General and administrative expenses | ||||||||||||||||
| Three Months Ended | Nine Months Ended | |||||||||||||||
| December 31, 2019 | December 31, 2018 | December 31, 2019 | December 31, 2018 | |||||||||||||
| $ | $ | $ | $ | |||||||||||||
| Salaries and benefits | 531 | 364 | 1,485 | 1,166 | ||||||||||||
| Professional fees | 725 | 244 | 1,862 | 935 | ||||||||||||
| Other | 317 | 152 | 1,017 | 412 | ||||||||||||
| Sub-total | 1,573 | 760 | 4,364 | 2,513 | ||||||||||||
| Stock-based compensation | 364 | 234 | 1,437 | 663 | ||||||||||||
| Total | 1,937 | 994 | 5,801 | 3,176 | ||||||||||||
| Sales and Marketing Expenses | ||||||||||||||||
| Three Months Ended | Nine Months Ended | |||||||||||||||
| December 31, 2019 | December 31, 2018 | December 31, 2019 | December 31, 2018 | |||||||||||||
| $ | $ | $ | $ | |||||||||||||
| Salaries and benefits | 482 | 96 | 1,081 | 217 | ||||||||||||
| Marketing | 14 | – | 750 | – | ||||||||||||
| Professional fees | 55 | 30 | 130 | 30 | ||||||||||||
| Other | 190 | 6 | 560 | 10 | ||||||||||||
| Sub-total | 741 | 132 | 2,521 | 257 | ||||||||||||
| Stock-based compensation | 109 | 28 | 285 | 67 | ||||||||||||
| Total | 850 | 160 | 2,806 | 324 | ||||||||||||
| 23 |
Three months ended December 31, 2019 compared to the three months ended December 31, 2018:
During the three months ended December 31, 2019, Acasti continued its planned advancement of the two-study TRILOGY Phase 3 clinical study program for its drug candidate, CaPre, in partnership with one of the world’s largest providers of biopharmaceutical development and clinical outsourcing services (“CRO”). R&D expenses before depreciation, amortization and stock-based compensation expense for the three months ended December 31, 2019 totaled $4,207 compared to $8,759 for the three months ended December 31, 2018. This $4,552 net decrease was mainly attributable to a $5,552 decrease in research contracts, partially offset by an increase in professional fees of $733 and an increase in salaries and benefits of $220 due to increased headcount. The lower research contract expense is attributed primarily to the advancement of the CRO as the Phase 3 clinical trial program is getting closer to completion.
G&A expenses totaling $1,573 before stock-based compensation expense for the three months ended December 31, 2019 and increased by $813 from $760 for the three months ended December 31, 2018. This increase was mainly attributable to an increase of $184 in the cost of our Directors and Officers insurance policy, as well as an increase of $481 in corporate, accounting and legal fees. Salaries and benefits also increased due to higher headcount and related benefits.
S&M expenses were $741 before stock-based compensation expense for the three months ended December 31, 2019 compared to $132 for the three months ended December 31, 2018. During the second quarter ended September 30, 2018, we hired our Chief Commercial Officer and we added to our sales and marketing team to support expanded business, market development and product launch activities.
The stock-based compensation expense increased by $273 to $609 for the three months ended December 31, 2019 from $336 for the three months ended December 31, 2018. The increase is mainly due to 2.3 million stock options granted to existing and new employees and directors during the nine months ended December 31, 2019, partially offset by stock options exercised, forfeited and expired. The weighted average fair value of the options granted to employees and directors during the nine months ended December 31, 2019 was $1.58, and no options were granted to consultants.
The depreciation and amortization expense remained relatively constant.
Net financial expenses for the three months ended December 31, 2019 was $7,873 compared to a financial gain of $6,100 for the three months ended December 31, 2018. The net increase in loss of $13,973 was mainly attributable to an increase in loss from the changes in fair value of derivative warrant liabilities of $7,748, partially offset by a lower number of warrants.
Nine months ended December 31, 2019 compared to the nine months ended December 31, 2018:
During the nine months ended December 31, 2019, Acasti continued its planned advancement of the two-study TRILOGY Phase 3 clinical study program for its drug candidate, CaPre, in partnership with its CRO. R&D expenses before depreciation, amortization and stock-based compensation expense for the nine months ended December 31, 2019 totaled $15,924, compared to $25,292 for the nine months ended December 31, 2018. This $9,368 net decrease was mainly attributable to a $10,742 decrease in research contracts, partially offset by an increase in salaries and benefits of $572 due to increased headcount and related benefits. The lower research contract expense is attributed primarily to the advancement of the CRO as the Phase 3 clinical trial program is getting closer to completion.
G&A expenses totaling $4,364 before stock-based compensation expense for the nine months ended December 31, 2019 and increased by $1,851 from $2,513 for the nine months ended December 31, 2018. This increase was mainly attributable to a $545 increase associated with our Directors and Officers insurance policy, as well as an increase of $927 in accounting, corporate and legal fees. Salaries and benefits also increased due to higher headcount.
S&M expenses were $2,521 before stock-based compensation expense for the nine months ended December 31, 2019 compared to $257 for the nine months ended December 31, 2018. During the second quarter ended September 30, 2018, we hired our Chief Commercial Officer and we added to our sales and marketing team to support expanded business, market development and product launch activities.
| 24 |
The stock-based compensation expense increased by $1,319 to $2,232 for the nine months ended December 31, 2019 from $913 for the nine months ended December 31, 2018. The increase is mainly due to 2.3 million stock options granted to existing and new employees and directors during the nine months ended December 31, 2019, partially offset by stock options exercised, forfeited and expired. The weighted average fair value of the options granted to employees and directors during the nine months ended December 31, 2019 was $1.58, and no options were granted to consultants.
The depreciation and amortization expense remained constant.
Net financial expenses for the nine months ended December 31, 2019 was $28,687 compared to net financial expenses of $3,689 for the nine months ended December 31, 2018. The net increase in loss of $24,998 was mainly attributable to an increase in the fair value of derivative warrant liabilities of $25,295, partially offset by a decrease in financing fees and a lower number of warrants.
Two separate derivative warrant liabilities are included in the statement of financial position as at December 31, 2019, and December 31, 2018. These derivative warrant liabilities stem from the financing transactions that took place in May 2018 and December 2017. The derivative warrant liabilities are re-measured at each reporting date using the Black-Scholes option pricing model. The valuations are mainly driven by the fluctuation in the Corporation’s stock price resulting in an increased or decreased loss or gain related to the change in fair value of the warrant liabilities and increasing or decreasing the corresponding liability in the statement of financial position.
| 25 |
SELECTED QUARTERLY FINANCIAL DATA
| December 31, | September 30, | June 30, | March 31, | |||||||||||||
| 2019 | 2019 | 2019 | 2019 | |||||||||||||
| $ | $ | $ | $ | |||||||||||||
| Net loss | (15,728 | ) | (28,343 | ) | (11,756 | ) | (16,806 | ) | ||||||||
| Add (deduct): | ||||||||||||||||
| Depreciation and amortization | 726 | 675 | 699 | 731 | ||||||||||||
| Stock based compensation | 609 | 1,298 | 325 | 128 | ||||||||||||
| Shares issued as legal settlement | – | – | – | 990 | ||||||||||||
| Financial expense (income) | 7,873 | 19,698 | 1,117 | 2,862 | ||||||||||||
| Non-IFRS operating loss | (6,520 | ) | (6,672 | ) | (9,615 | ) | (12,095 | ) | ||||||||
| Basic and diluted net loss per share | (0.07 | ) | (0.08 | ) | (0.12 | ) | (0.22 | ) |
| December 31, | September 30, | June 30, | March 31, | |||||||||||||
| 2018 | 2018 | 2018 | 2018 | |||||||||||||
| $ | $ | $ | $ | |||||||||||||
| Net loss | (4,610 | ) | (22,729 | ) | (7,421 | ) | (8,140 | ) | ||||||||
| Add (deduct): | ||||||||||||||||
| Depreciation and amortization | 723 | 689 | 684 | 667 | ||||||||||||
| Stock based compensation | 336 | 326 | 251 | 268 | ||||||||||||
| Financial expense (income) | (6,100 | ) | 12,291 | (2,502 | ) | 778 | ||||||||||
| Non-IFRS operating loss | (9,651 | ) | (9,423 | ) | (8,988 | ) | (6,427 | ) | ||||||||
| Basic and diluted net loss per share | (0.07 | ) | (0.62 | ) | (0.23 | ) | (0.32 | ) |
The quarterly year-to-year non-IFRS operating loss variances are mainly attributable to fluctuations in R&D expenses associated with the TRILOGY Phase 3 clinical trial program from quarter-to-quarter, as well as an increase in G&A and S&M expenses over the last four quarters as the Corporation increased back-office administrative resources and added new commercial team members to manage its commercialization and marketing efforts.
| 26 |
LIQUIDITY AND CAPITAL RESOURCES
Share Capital Structure
The Corporation’s authorized share capital consists of an unlimited number of Class A, Class B, Class C, Class D and Class E shares, without par value. Issued and outstanding fully paid shares, stock options, restricted shares units and warrants, were as follows for the periods ended:
| December 31, 2019 | March 31, 2019 | |||||||
| Number outstanding | Number outstanding | |||||||
| Class A shares, voting, participating and without par value | 89,057,819 | 78,132,734 | ||||||
| Stock options granted and outstanding | 6,277,152 | 4,046,677 | ||||||
| May 2018 public offering of warrants exercisable at $1.31, until May 9, 2023 | 6,593,750 | 10,188,100 | ||||||
| Public offering broker warrants May 2018 exercisable at $1.05 until May 9, 2023 | 222,976 | 547,975 | ||||||
| December 2017 U.S. public offering of warrants exercisable at US$1.26, until December 27, 2022 | 7,072,962 | 9,801,861 | ||||||
| December 2017 U.S. broker warrants exercisable at US$1.2625, until December 27, 2022 | 259,121 | 495,050 | ||||||
| February 2017 public offering of warrants exercisable at $2.15, until February 21, 2022 | 1,723,934 | 1,904,034 | ||||||
| 2017 unsecured convertible debentures conversion option contingent warrants exercisable at $1.90, until February 21, 20203 | 902,630 | 1,052,630 | ||||||
| Total fully diluted shares | 112,110,344 | 106,169,061 |
Cash Flows and Financial Condition between the three and nine-month periods ended December 31, 2019 and 2018
Summary
As at December 31, 2019, cash and cash equivalents totaled $25,678, a net decrease of $134 and a net increase of $3,157 for the three and nine-month periods ended December 31, 2019, respectively. This compares to cash and cash equivalents totaling $28,893 at December 31, 2018, and a net increase of cash totaling $22,924 and $20,670 for the three and nine-month periods ended December 31, 2018, respectively.
Operating activities
During the three months ended December 31, 2019 and December 31 , 2018, the Corporation’s operating activities used cash of $9,197 and $9,966, respectively, and during the nine-months periods ended December 31, 2019 and December 31, 2018, the Corporation’s operating activities used cash of $26,678 and $22,146 respectively, further modified by changes in working capital, excluding cash. The difference between the use of cash flows in operating activities for the three and nine-months periods ended December 31, 2019 and 2018, when compared to the net losses for each period is mainly attributable to the change in non-cash expenses, (see “Reconciliation of Net Loss to Non-IFRS Operating Loss”), further modified by changes in working capital, excluding cash.
_______________________
3 The debentures are convertible into Common Shares at a fixed price of $1.90 per Common Share except if the Corporation pays before the maturity, all or any portion of the convertible debentures.
| 27 |
Investing activities
During the three months ended December 31, 2019, the Corporation’s investing activities used cash of $268, primarily due to the acquisition of equipment, compared to a use of cash of $16,820 for the three months ended December 31, 2018, due mostly to the acquisition of marketable securities.
During the nine months ended December 31, 2019, the Corporation’s investing activities provided cash of $11,846 primarily due to the maturity of marketable securities, compared to a use of cash of $17,284 for the nine months ended December 31, 2018 due mostly to the acquisition of marketable securities.
Financing activities
During the three months ended December 31, 2019, the Corporation’s financing activities provided net cash totaling $9,452 due primarily to shares sold via the ATM program for a total of approximately $8.0 million, and the exercise of warrants for a total of approximately $1,5 million. During the three months ended December 31, 2018, the Corporation generated cash of $49,034 due primarily to the net proceeds from the public offerings of $48,024, and proceeds from warrants exercised related to the May 2018 public offering of $1,011.
During the nine months ended December 31, 2019, the Corporation’s financing activities generated cash of $18,112 mainly from shares sold via the ATM program for a total of approximately $8.0 million, and the exercise of warrants for a total of approximately $10.0 million. During the nine months ended December 31, 2018, the Corporation’s financing activities generated cash of $59,345 mainly from the net proceeds of the public offerings of $58,337 and proceeds from warrants exercised related to the May 2018 public offering of $1,011.
ATM Program
On February 14, 2019, the Corporation entered into an “at-the-market” (“ATM”) sales agreement with B. Riley FBR, Inc., pursuant to which the Corporation’s common shares may be sold from time to time for aggregate gross proceeds of up to US $30 million, with sales only being made on the NASDAQ Stock Market. The common shares may be distributed at market prices prevailing at the time of any sale and, as a result, prices may vary between purchasers and during the period of distribution. As at December 31, 2019, a total of 2.9 million shares had been sold for total net proceeds of approximately $8.0 million, in relation to the ATM. As at December 31, 2019, costs incurred in connection to the ATM amounted to $261 and were recorded as deferred financing while proportional costs related to the shares sold for a total of $28 were debited to Equity.
October 2018 Public Offering
On October 9, 2018, the Corporation closed a U.S. public offering of 16,600,000 Common Shares at a price of US$1.00 per share. In addition, the underwriters fully exercised their over-allotment option to purchase 2,490,000 additional Common Shares at the same public offering price. This offering generated gross proceeds of $24.7 million (US$19.1 million), which resulted in net proceeds to the Corporation of $22.6 million (US$17.4 million) and a total of 19,090,000 Common Shares issued.
On October 23, 2018, the Corporation closed a Canadian public offering of 18,750,000 Common Shares at a price of $1.28 per share. In addition, the underwriters fully exercised their over-allotment option to purchase 2,812,500 additional Common Shares at the same public offering price. This offering generated gross proceeds of $27.6 million, which resulted in net proceeds to the Corporation of approximately $25.4 million and a total of 21,562,500 Common Shares issued.
May 2018 Public Offering
On May 9, 2018 the Corporation closed a Canadian public offering issuing 9,530,000 units of Acasti (“Units”) at a price of $1.05 per Unit for gross proceeds of $10 million. The units issued consist of 9,530,000 Common Shares and 9,530,000 Warrants. Each Warrant entitles the holder thereof to acquire one Common Share of the Corporation at an exercise price of $1.31 at any time until May 9, 2023.
| 28 |
On May 14, 2018, the underwriters exercised their over-allotment option by purchasing an additional 1,429,500 units at a price of $1.05 per Unit, for additional gross proceeds of $1.5 million. The units issued consist of 1,429,500 Common Shares and 1,429,500 warrants. Each Warrant entitles the holder thereof to acquire one Common Share of the Corporation at an exercise price of $1.31 at any time until May 9, 2023.
The warrant component of these Units are Derivative Warrant Liabilities for accounting purposes due to the warrant agreement, which contains certain contingent provisions that allow for cash settlement. The proceeds of the offering are required to be split between the Derivative Warrant Liabilities and the equity-classified Common shares at the time of issuance of the Units. The fair value of the Derivative Warrant Liabilities at the time of issuance was determined to be $4.3 million and the residual of the proceeds of $6.2 million was allocated to the Common Shares. Issuance costs related to this transaction totaled approximately $1.8 million and have been allocated between the Derivative Warrant Liabilities and Common shares based on relative value. Resulting from this allocation, $0.7 million has been allocated to the Derivative Warrant Liability and is recognized in finance costs in the Statements of Earnings and Comprehensive Loss, whereas the remaining portion of $1.1 million in issuance costs was allocated to the Common Shares and recognized as a reduction to share capital, in the Statements of Financial Position.
The weighted average fair value of the 2018 Warrants issued in May 2018 was determined to be $0.39 per warrant. Changes in the fair value of the 2018 Warrants are recognized in finance expense.
As part of the May financing, the Corporation also issued broker warrants to purchase up to 547,975 Common Shares. Each broker warrant entitles the holder thereof to acquire one Common Share of the Corporation at an exercise price of $1.05, at any time until May 9, 2023. The broker warrants are considered for compensation to non-employees under IFRS 2, stock-based compensation, and are accounted for at fair value at issuance date and not subsequently revalued.
| 29 |
Financial Position
The following table details the significant changes to the statements of financial position as at December 31, 2019 compared to the prior fiscal period end at March 31, 2019:
| Accounts | Increase (Decrease) | Comments | ||||
| Cash and cash equivalents | 3,157 | See cash flow statement | ||||
| Marketable securities | (11,866 | ) | Progression of research contracts | |||
| Receivable | (30 | ) | Timing of receipts | |||
| Deferred Financing Costs | 82 | Additional accounting and legal fees incurred in connection with the ATM program, net of expenses applied to Equity | ||||
| Prepaid expenses | 793 | Advances to vendors, including insurance policy, net of amortization | ||||
| Equipment | 28 | Acquisition of equipment net of depreciation | ||||
| Intangible asset | (1,742 | ) | Amortization | |||
| Trade and other payables | (4,086 | ) | Timing of payments net of accruals and settlement of provision for legal settlement via the issuance of common shares | |||
| Derivative warrant liabilities | 14,495 | Change in fair value and exercise of derivative warrants | ||||
| Unsecured convertible debentures | 141 | Accretion of interest | ||||
See the statement of changes in equity in the Corporation’s financial statements for details of changes to the equity accounts since March 31, 2019.
Treasury Operations
The Corporation’s treasury policy is to invest cash that is not required immediately into instruments with an investment strategy based on capital preservation. Cash equivalents and marketable securities are primarily made in guaranteed investment certificates (GICs), term deposits and high-interest savings accounts, which are issued and held with Canadian chartered banks; high rated promissory notes issued by government bodies and commercial paper. The Corporation holds cash denominated in both US and CAD dollars. Funds received in US dollars from the equity private placement are invested as per the Corporation’s treasury policy in US dollar investments and converted to CAD dollars as appropriate to fulfill operational requirements and funding.
Derivative warrant liabilities
The 10,188,100 Warrants issued as part of the Corporation’s May 2018 public offering were recognized as Derivative Warrant Liabilities with a fair value of $4,272. During the nine months ended December 31, 2019, a total of 3,594,350 warrants were exercised. As of December 31, 2019, the Derivative Warrant Liability for the remaining 6,593,750 Warrants totaled $15,405, which represents the fair value of these warrants. The weighted average fair value of the 2018 Warrants issued was determined to be $0.39 per warrant at inception and approximately $2.33 per warrant as at December 31, 2019.
On December 27, 2017, 9,801,861 warrants were issued as part of the Corporation’s U.S. public offering and recognized as Derivative Warrant Liabilities with a fair value of $5,873 (“2017 Warrants”). The 2017 Warrants are Derivative Warrant Liabilities for accounting purposes due to the currency of the exercise price (US$) being different from the Corporation’s Canadian dollar functional currency. During the nine months ended December 31, 2019, 2,728,899 warrants were exercised (including 52,288 warrants exercised in a cashless manner). As of December 31, 2019, the Derivative Warrant Liability for the remaining 7,072,962 Warrants totaled $15,353, which represents the fair value of these warrants. The weighted average fair value of the 2018 Warrants issued was determined to be $0.60 per warrant at inception and approximately $2.17 per warrant as at December 31, 2019.
| 30 |
The increase in the fair value of both existing derivative warrant liabilities as at December 31, 2019 is due to the increase in the Corporation’s share price and the dilution factor.
During the period from June to December 31, 2019, the following warrants were exercised with the resulting cash proceeds:
| Number exercised | Proceeds | |||||||
| $ | ||||||||
| May 2018 over-allotment Warrants 2018 | 3,594,350 | 4,709 | ||||||
| Series December 2017 US Public offering Warrants 2017 | 2,676,611 | 4,470 | ||||||
| Public offering warrants February 2017 | 180,100 | 387 | ||||||
| Public offering Broker warrants May 2018 | 325,000 | 341 | ||||||
| Contingent warrants private placement 2017 | 150,000 | 285 | ||||||
| 6,926,061 | 10,192 |
In addition, 235,929, broker warrants and 52,288 derivative warrants offered as part of the December 2017 U.S. public offering were exercised in a cashless manner to acquire 136,013 Common Shares of Acasti.
During the three-month and nine-month periods ended December 31, 2018, 771,400 warrants offered as part of the May 2018 public offering were exercised at an exercise price of $1.31 per Common Share of the Company, resulting in $1.0 million of cash proceeds. In addition, 4,455 warrants offered as part of the December 2017 U.S. public offering were exercised in a cashless manner to acquire 1,074 Common Shares of the Company. A total of 772,474 Common Shares were issued as a result of 775,855 warrants being exercised.
Contractual Obligations, Off-Balance-Sheet Arrangements and Commitments
As at December 31, 2019, the Corporation’s liabilities total $45,059, of which $12,343 is due within twelve months, $30,758 relates to Derivative Warrant Liabilities that will be settled in Common Shares and $1,958 of outstanding unsecured convertible debentures is also projected to be settled in Common Shares. However, the principal amount of unsecured convertible debentures may be prepaid, in whole or in part, at any time and from time to time, in cash, at the sole discretion of the Corporation. The debentures are convertible into Common Shares at a fixed price of $1.90 per Common Share except if the Corporation pays before the maturity, all or any portion of the convertible debentures.
A summary of the contractual obligations at December 31, 2019, is as follows:
| Carrying value | Total contractual cash flows | 1 year or less | 1 to 3 years | |||||||||||||
| $ | $ | $ | $ | |||||||||||||
| Trade, other payables and due to related party | 12,343 | 12,343 | 12,343 | – | ||||||||||||
| Lease | 19 | 19 | 19 | – | ||||||||||||
| Unsecured convertible debentures | 1,958 | 2,000 | 2,000 | – | ||||||||||||
| Total | 14,320 | 14,362 | 14,362 | – |
RKO supply agreement
On October 25, 2019, the Corporation signed a supply agreement with Aker Biomarine Antartic AS (AKER), to purchase raw krill oil product (RKO) for a committed volume of commercial starting material for CaPre for a total value of USD $3.1 million. The delivery of the product has been established following a calendar year basis and it is expected to be completed in the first half of FY2021. As at December 31, 2019, the remaining balance of the commitment with AKER amounts to USD $2.9 million.
| 31 |
Research and development contracts and contract research organizations agreements
The Corporation utilizes Contract Manufacturing Organizations (CMOs) for the development and production of clinical materials and contract research organizations to perform services related to the Corporation’s clinical trials. Pursuant to the agreements with these CMOs and contract research organizations, the Corporation has either the right to terminate the agreements without penalties or under certain penalty conditions.
Lease
During Fiscal 2018, the Corporation entered into a lease agreement, for its research and development and quality control laboratory facility located in Sherbrooke, Québec, resulting in a commitment of $19 over the remaining three months of the lease term.
Contingencies
The Corporation evaluates contingencies on an ongoing basis and establishes loss provisions for matters in which losses are probable and the amount of the loss can be reasonably estimated.
On May 10, 2019, the Corporation announced the settlement regarding legal claims made by its former chief executive (“CEO”) officer with respect to the termination of his employment. Pursuant to the settlement agreement, the Corporation agreed to issue 900,000 common shares at $1.10 per share to the former CEO. In addition, the Corporation agreed to reimburse the former CEO for legal fees of $64. Furthermore, pursuant to the settlement agreement, the Corporation received a full and final release from the former CEO on all procedures in connection with the termination of his employment. This settlement was accrued as a short-term liability as at March 31, 2019 and the expense of $1,054 was included as part of General and administrative expenses. During May 2019, the shares were issued and the liability of $990 reclassified as Equity.
Related Party Transactions
The key management personnel are the officers of the Corporation and the members of the Board of Directors of the Corporation. They control collectively less than 1% of the voting shares of the Corporation. See note 6 to the financial statements for disclosures of key management personnel compensation.
| 32 |
Controls and procedures
In accordance with the Canadian Securities Administrators’ National Instrument 52-109, the Corporation has filed certificates signed by the Corporation’s Chief Executive Officer (“CEO”) and Vice President Finance that among other things, report on the design of disclosure controls and procedures and the design of internal control over financial reporting.
Disclosure controls and procedures
The CEO and Vice President Finance, have designed disclosure controls and procedures, or has caused them to be designed under their supervision, in order to provide reasonable assurance that:
| · | material information relating to the Corporation has been made known to them; and |
| · | information required to be disclosed in the Corporation’s filings is recorded, processed, summarized and reported within the time periods specified in securities legislation. |
Changes in internal control over financial reporting (“ICFR”)
During the nine months ended December 31, 2019, we implemented a new fully integrated, scalable, Enterprise Resource Planning (“ERP”) system “Navision”, to replace our former accounting system. Navision went live on April 1, 2019 and it has been used to record our transactions and produce our financial and operating reports. Certain of the Corporation’s controls have been amended to reflect the new ERP system.
There have been no other changes in the Corporation’s ICFR during the three months ended September 30, 2019 that have materially affected or are reasonably likely to materially affect its ICFR.
Upcoming Changes in IFRS / Foreign Private Issuer Status
Under the Securities Exchange Act of 1934 (“Exchange Act”), a foreign private issuer (“FPI”) is an entity incorporated or organized under the laws of a jurisdiction outside of the U.S., unless:
| • | more than 50% of its outstanding voting securities are directly or indirectly owned of record by U.S. residents; and | |
| • | any of the following applies: (i) the majority of its executive officers or directors are U.S. citizens or residents; (ii) more than 50% of its assets are located in the U.S.; or (iii) its business is administered principally in the U.S. |
A corporation’s ongoing FPI status is tested annually at the end of the most recently completed second fiscal quarter. If an issuer fails to qualify as an FPI at the end of its second fiscal quarter, it remains eligible to use the forms and rules applicable to FPIs until the end of that financial year. Historically, we met the definition of an FPI, and as such, prepared consolidated financial statements in accordance with IFRS, reported with the United States Securities and Exchange Commission (“SEC”) on FPI forms, and complied with SEC rules and regulations applicable to FPIs.
As of September 30, 2019, due to an increase
in the percentage of its Common Shares held by U.S. residents above 50%, the Corporation has determined that it no longer qualifies
as an FPI. Therefore, the Corporation plans to transition to U.S. domestic corporation reporting status and become subject to SEC
reporting requirements applicable to a U.S. domestic corporation, beginning on April 1, 2020. These reporting requirements will
require that the Corporation’s fiscal 2020 financial statements be recast into United States Generally Accepted Accounting
Principles for all periods presented, which will include the fiscal 2019 comparative financial information. Therefore, the last
period under which the Corporation will report under IFRS is the third quarter ended December 31, 2019. The extent of the impact
of this transition has not yet been determined. In addition, the Corporation will be required to file Form 10-K annual, Form 10-Q
quarterly and Form 8-K current reports with the SEC, its insiders will have to comply with U.S. insider filing requirements under
the Exchange Act, and the Corporation will become subject to the SEC’s proxy rules.
| 33 |
RISK FACTORS
Investing in Acasti’s securities involves a high degree of risk due to, among other things, the nature of our business and the present stage of our development. Prospective and current investors should carefully consider the following risks and uncertainties, together with all other information in this MD&A, as well as our financial statements and the risks described in more detail in Item 3. “Risk Factors” and “Item 5. Operating and Financial Review and Prospects” in our Annual Report on Form 20-F for the fiscal year ended March 31, 2019 and our other public filings. If any of these risks actually occur, Acasti’s business, financial condition, prospects, results of operations or cash flow could be materially and adversely affected and all or a part of the value of an investor’s investment in Acasti can be lost. Additional risks or uncertainties not currently known to Acasti, or that we currently deem immaterial, may also negatively affect our business operations.
General Risks Related to the Corporation
| · | We may not be able to maintain our operations and advance our research and development of CaPre without additional funding. |
| · | We may never become profitable or be able to sustain profitability. |
| · | While the REDUCE-IT results (a Cardiovascular outcome study conducted by Amarin with their OM3 drug VASCEPA) were positive, on January 13, 2020 AstraZeneca announced that its cardiovascular Phase 3 STRENGTH trial for their OM3 drug EPANOVA had been discontinued due to its low likelihood of demonstrating a benefit to patients with mixed dyslipidaemia (MDL). The potential impact of the discontinuance of the STRENGTH trial on Acasti’s business and the OM3 drug market in general are not yet known. |
| · | We are and will continue to rely on third parties to conduct our TRILOGY Phase 3 program for CaPre. |
| · | We rely on third parties to manufacture, produce and supply CaPre and we may be adversely affected if those third parties are unable or unwilling to fulfill their obligations, including complying with FDA requirements. |
| · | We have historically had no marketing and sales organization and, as a corporation, no history in marketing products. If we are unable to properly establish marketing and sales capabilities or enter into agreements with a strategic partner to market and sell CaPre, we may not be able to generate revenue. |
| · | If we are not successful in attracting and retaining highly qualified personnel, we may not be able to successfully implement our business strategy. |
| · | Business disruptions could seriously harm our future revenue and financial condition and increase our costs and expenses. |
| · | Our prospects currently depend entirely on the success of CaPre, which is still in clinical development, and we may not be able to generate revenues from CaPre. |
| · | Our TRILOGY Phase 3 program for CaPre may not achieve all or any of its primary and secondary endpoints. |
| · | Our investigations into the unusually large placebo effect seen in our triglyceride topline data in our TRILOGY 1 clinical trial may not produce any meaningful explanations, and there is no assurance that any explanation can lead to an adjusted primary endpoint for TRILOGY 1 that achieves statistical significance or a positive trend in favor of Capre in a manner supported by the FDA. |
| · | Based on the final TRILOGY 1 and TRILOGY 2 data, the FDA may require that we conduct additional clinical work to support an NDA for CaPre. |
| · | We may not be able to obtain required regulatory approvals for CaPre. |
| · | Even if we receive regulatory approval for CaPre, it may just be for a limited indication. |
| · | We may be unable to find successful strategic partnerships to develop and commercialize CaPre. |
| · | We may be unable to develop alternative product candidates. |
| · | We may not be able to compete effectively against our competitors’ pharmaceutical products. |
| 34 |
| · | CaPre could face competition from products for which no prescription is required. |
| · | Recent and future legal developments could make it more difficult and costly for us to obtain regulatory approvals for CaPre and negatively affect the prices we may charge. |
| · | Reimbursement decisions by third-party payors may have an adverse effect on pricing and market acceptance. If there is not sufficient reimbursement for CaPre, it is less likely that it will be widely used. |
| · | Even if we obtain FDA approval of CaPre, we may never obtain approval or commercialize it outside of the United States, which would limit our ability to realize CaPre’s full market potential. |
| · | If we or our third-party service providers fail to comply with healthcare laws and regulations or government price reporting laws, we could be subject to civil or criminal penalties. | |
| · | The research, development and manufacture of CaPre involves using potentially hazardous materials. |
| · | If CaPre reaches commercialization, interruptions of our supply of CaPre could impair any future revenue streams. |
| · | If product liability lawsuits are brought against us, we may incur substantial liabilities and be required to cease the sale, marketing and distribution of CaPre. We may not achieve our publicly announced milestones on time, or at all. |
| · | We may be subject to foreign exchange rate fluctuations. |
| · | While there is no indication of this in previous studies, CaPre may cause or be perceived to cause undesirable side effects or have other properties that could delay or prevent its regulatory approval, limit the commercial profile of an approved label, or result in significant negative consequences following marketing approval, if any. |
Risks Related to Intellectual Property
| · | In addition to our own patents, CaPre is covered by patents that are sublicensed to us by Neptune. |
| · | It is difficult and costly to protect our intellectual property rights. |
| · | CaPre may infringe the intellectual property rights of others, which could increase our costs and delay or prevent our development and commercialization efforts. |
| · | If we do not protect our trademark for CaPre, we may not be able to build name recognition in our markets of interest. |
| · | We may be involved in lawsuits to protect or enforce our patents or the patents of our licensors, which could be expensive, time-consuming and unsuccessful. |
| · | Changes in patent law could diminish the value of patents in general, thereby impairing our ability to protect CaPre and any of our other future product candidates. |
| · | We may not be able to protect our intellectual property rights throughout the world. |
Risks Relating to Our Common Shares
| · | The price of our common shares may be volatile. |
| · | Forward-Looking Statements may prove to be inaccurate. |
| · | Raising additional capital may cause dilution to our existing shareholders, restrict our operations or require us to relinquish rights to our technologies or product candidates. |
| · | There can be no assurance that an active market for our common shares will be sustained. |
| · | A large number of common shares may be issued and subsequently sold upon the exercise of existing warrants. The sale or availability for sale of existing warrants or other securities convertible in common shares may depress the price of our common shares. |
| · | We do not currently intend to pay any cash dividends on our common shares in the foreseeable future. |
| · | If we fail to meet applicable listing requirements, the NASDAQ Stock Market or the TSXV may delist our common shares from trading, in which case the liquidity and market price of our common shares could decline. |
| · | We may pursue opportunities or transactions that adversely affect our business and financial condition. |
| · | As a “non-accelerated filer”, we are not required to comply with the auditor attestation requirements of the Sarbanes-Oxley Act. |
| · | U.S.
investors may be unable to enforce certain judgments. |
| 35 |
Additional Information
Updated and additional information about the Corporation is available on SEDAR at www.sedar.com or on EDGAR at www.sec.gov/edgar.shtml.
As at February 13, 2020 the Corporation’s capital structure is as follows:
| Number outstanding | ||||
| Class A shares, voting, participating and without par value | 90,209,449 | |||
| Stock options granted and outstanding | 6,277,152 | |||
| May 2018 public offering of warrants exercisable at $1.31, until May 9, 2023 | 6,593,750 | |||
| Public offering broker warrants May 2018 exercisable at $1.05 until May 9, 2023 | 222,976 | |||
| December 2017 U.S. public offering of warrants exercisable at US$1.26, until December 27, 2022 | 7,072,962 | |||
| December 2017 U.S. broker warrants exercisable at US$1.2625, until December 27, 2022 | 259,121 | |||
| February 2017 public offering of warrants exercisable at $2.15 until February 21, 2022 | 1,723,934 | |||
| 2017 unsecured convertible debentures conversion option | ||||
| contingent warrants exercisable at $1.90, until February 21, 20204 | 902,630 | |||
| Total fully diluted shares | 113,261,974 |
______________________
4 The debentures are convertible into Common Shares at a fixed price of $1.90 per Common Share except if the Corporation pays before the maturity, all or any portion of the convertible debentures.
36